Download

1 / 24
250 likes | 487 Views
CORYNEFORM BACTERIA. Diphteroids. Pleomorphic gram-positive rods. Club Shaped ( Chinese Letter like, V forms ) Catalase +ve Non sporing Non acid fast. Diphteroids (Continued). Commensals of the throat and skin of low pathogenicity.

E N D
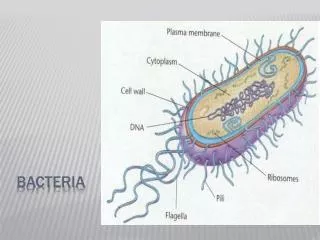
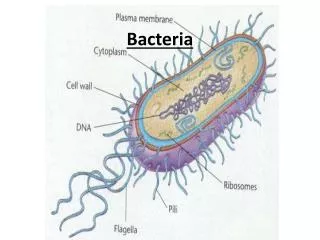
Diphteroids • Pleomorphic gram-positive rods. • Club Shaped (Chinese Letter like, V forms) • Catalase +ve • Non sporing • Non acid fast
Diphteroids (Continued) • Commensals of the throat and skin of low pathogenicity. • Morphologically similar to the pathogenic C.diphtheriae. • Can be found as contaminants of blood cultures and CSF. • Can cause opportunestic infections in Immunosupressed patients.
Corynebacterium diphtheriae (diphtheria) • Local infection of the throat with grayish adherent exudate (Pseudomembrane) and generalized toxaemia due to production and dissemination of a highly potent toxin.
Etiology Corynebacterium diphtheriae 3 Types of Colony: • Mitis (Mild disease) • Intermedius (Intermediate dis.) • Gravis (severe) • Strains may be toxegenic or non-toxegenic. • Production of toxin is mediated by bacteriophage (β phage) infection of the bacterium.
Etiology Corynebacterium diphtheriae (Continued) • The demonstration of toxin production is essential to differentiate toxegenic from commensal corynebacteria. • Toxogenicity is demonstrated by the agar gel precipitation (Elek) test or by the polymerase chain reaction (PCR).
Clinical Manifestation Usually gradual onset of local infection. • Membranous nasopharyngitis • Obstructive laryngotrachitis • With low grade fever • Malaise • Fatigue • Sore throat
Clinical Manifestation (Continued) Clinically: • Nasal diph. thick nasal discharge (intoxication rare) • Pharyngial thick, adherent pseudomembrane (intoxication common) • (tonsillar) Odema, Heat + Tenderness of tissue of neck (Bull neck) • Laryngial extension of membrane (asphyxia)
Clinical Manifestation (Continued) Less Commonly: • Cutanous • Vaginal • Conjunctival or otic
Clinical Manifestation (Continued) Life threating complication include: • Upper airway obstruction (extension of membrane) • Myocarditis (heart failure) • Neurologic Peripheral neuritis • Vocal cord paralysis • Ascending paralysis • Difficulty in swallowing • Visual disturbance
Epidemiology • Humans are the only reservoir. • Sources of Infections: • Discharges from nose, throat, eye and skin lesions of infected patients or carriers (direct contact) • Most common in low socioeconomic groups in crowded conditions. • Since 1990 – epidemics in Soviet Union, Russia with 50,000 cases – 1750 deaths.
Epidemiology (Continued) • Case fatality 3% - 23% • Children are susceptable after 3-6 months (highest incidence). • Latent skin infection immunity. • Communicability 2 weeks (untreated person) <4 days (treated patients) • Incubation Period is 2- 5 days.
Pathogenesis Powerful exotoxin ( blood stream): • Toxin local and systemic toxicity (toxin mediated disease) • Cause of mortality in clinical diphtheria. • Affinity for heart muscles, nerve endings and adreral glands. • Produced by β phage infected C.diphtheriae.
Pathogenesis (Continued) • Rapidly diffused from local lesion irreversibly bound to tissues. • ADP ribosylating toxin protein synthesis inhibition cell death necrosis and neutroxic effects. • Bacilli (local effect), no deep penetration to blood or underlying tissue. • Inflammatory exudate and necrosis of pharyngeal muscles respiratory obstruction.
Diagnosis Clinical diagnosis: • Lab should not delay management. • Specimen for culture • Nose From both • Throat Patient and carrier • Lesions
Elek plate demonstrating toxin from Corynebacterium diphtheriae
Diagnosis (Continued) Direct stained smear unreliable (Commensals) • Special media (Potassium -tellurite) and enriched Loefflers slope (selective) grey black colonies. • Albert stain metachromatic granules. • Toxogenicity test (Elek test, PCR) is most important, guinea pig inoculation. • Elek test: agar gel precipitation.
Management Patient: • Fatality with delay (0 -20%) 1- Antitoxin • Equine antitoxin – neutralize the toxin • Start soon if clinically suspected. 2- Isolation of the patient (droplet precautions) 3- Antibiotics (no effect on toxin) to eradicate organism and prevent spread (a) Penicillin – oral (b) Erythromycin
Management (Continued) 3- Contacts (Close) • Investigated for signs of disease Carriage (nose, throat) • Chemoprophylaxis (erythromycin) • Immunization of susceptiable contacts (diph. toxoid) • Carriers isolated and treated.
Prevention and Control • Universal immunization with diph. toxoid the only effective control measure. • High immunization rate among children (3 doses of DPT + 2 boosters at 2 month age) • Regular booster (Td every 10 years). • Vaccine = formalin treated toxin – highly antigenic, not toxic.
Listeriamonocytogenes • Listeriamonocytogenes is widespread in nature and has been • isolated from the stools of 5% healthy adults. A variety of foods are contaminated with LM. It has been recovered from raw vegetables, raw milk, fish, poultry, soft cheese and meats at • rates ranging from 15% to 70%
Resistance to LM infection is predominantly cell-mediated Evidence of this is provided by the overwhelming clinical • association between Listeria infections and conditions associated with impaired cellular immunity, including lymphomas, pregnancy, AIDS and corticosteroid-induced immunosupression in transplant recipients.
Listeriamonocytogenes (LM) meningitis is rare in patients with a normal immune status. Most reported cases have been associated with immunosupression produced by drugs (steroids and cytotoxic drugs), chronic renal disease, diabetes, malignancy • and HIV . Additional groups include neonates , pregnant women and elderly