Download
1 / 49
590 likes | 1.42k Views
Principles of Drug Action. Prinsip-prinsip aksi obat Sugiyanto Lab. Farmakologi & Toksikologi Fak . Farmasi UGM. General Overview.

E N D
Principles of Drug Action Prinsip-prinsipaksiobat Sugiyanto Lab. Farmakologi & Toksikologi Fak. Farmasi UGM
General Overview • A few drugs act by virtue of their physicochemical properties, e.g. laxative agent (MgSO4), general anesthetics (based on its lipid solubility (?), osmotic diuretics (mannitol) • Some drugs act as false substrates (sulphonamides) or inhibitor for certain transport systems (cardiac glycosides) or enzymes (NSAIDs) • Most drugs produce their effects by acting on specific protein molecules, usually located in the cell membrane. These proteins are called receptors
Receptor, Agonist & Antagonist • Receptors normally respond to endogenous chemicals in the body. • These chemicals are either synaptic transmitter substances (neurotransmitters) or hormones, for example acetylcholine, epinephrine, insulin, aldosterone etc. • Chemicals or drugs that activate receptors and produce a response are called agonist. • Drugs or chemicals that combine to receptors but do not activate them are called antagonist
Receptors • They are protein molecules which are normally activated by neurotransmitters or hormones. • Many receptors have now been cloned and their amino acid sequences determined. • The 4 main type of receptors are: • 1. Agonist-gated receptors are made up from subunits which form a central ion channel (e.g. nicotinic receptor) • 2. G-protein-coupled receptors form a family of receptors with seven membrane-spanning helices
Receptors • 3. Nuclear Receptors (Intracellular receptors, Protein Synthesis-regulating Receptors) for steroid hormones and thyroid hormones • 4.Kinase-linked receptors (Ligand-regulated Enzymes) adalah reseptor permukaan membran yg biasanya mempunyai aktivitas kinase tirosin intrinsik, sebagai contoh: reseptor insulin, reseptor sitokin dan reseptor faktor pertumbuhan
Reseptorasetilkolinnikotinik : • Suatu protein pentamer yang terdiri dari 5 subunit yaitu 2βγδ • Terkait dengan kanal Na+ • berlokasi di neuromuscular junction, ganglia otonom, medula adrenal, dan CNS • pertama kali dikarakterisasi dengan kemampuannya mengikat nikotin
Contohreseptorterkopel protein G • Reseptor asetilkolin muskarinik • Reseptor adrenergik • Reseptor dopamin • Reseptor angiotensin
Reseptor terkopel Protein G • merupakan keluarga terbesar reseptor permukaan sel • menjadi mediator dari respon seluler berbagai molekul, seperti: hormon, neurotransmiter, mediator lokal, dll. • merupakan satu rantai polipetida tunggal, keluar masuk menembus membran sel sampai 7 kali disebut memiliki 7 transmembran
Some examples of Nuclear Receptor (Protein synthesis-regulating Receptors)
ContohKinase-linked Receptor (Ligand-regulated Enzymes) Reseptor Insulin
Drug-receptor Interactions • The activation of receptors by an agonist is coupled to the physiological or biochemical responses by transduction mechanisms that often (but not always) involve molecules called second messengers (for example Ca2+, inositol triphosphate, diacylglycerol and cAMP) • The interaction between a drug and the binding site of the receptor depends on the complementary of “fit” of the 2 molecules. • The closser the fit and the grater the number of bonds (usually non-covalent), the stronger will be the attractive forces between them, and the higher the affinity of the drug for the receptor.
Aktivasi GPCR (G protein-coupled receptor) melaluisistemfosfolipase • merupakan salah satu mekanisme transduksi signal yang penting • diawali dg pengikatan suatu ligan pada reseptor mengaktivasi enzim fosfolipase C membelah PIP2menjadi IP3dan DAG • PIP2 = fosfatidil inositol bis-fosfat merupakan hasil degradasi fosfatidil inositol pada membran sel dg bantuan enzim PI kinase • IP3= inositol trifosfat berikatan dengan reseptor spesifik pada retikulum endoplasmik yang tekait dg kanal Ca++ memicu pelepasan kalsium intrasel kontraksi sel, pelepasan hormon/neurotransmiter, eksositosis • DAG = diasil gliserol mengaktivasi protein kinase C memfosforilasi residu serine/threonin kinase pada sel target
Signal molecule PI 4,5-biphosphate (PI(4,5)P2) G-protein linked receptor Activated Phospholipase Cb diacylglycerol Activated PKC Activated G a subunit inositol 1,4,5-triphosphate (IP3) Ca++ Open IP3-gated Ca++ channel lumen of endoplasmic reticulum
Specificity & selectivity • The ability of a drug to combine with one particular type of receptor is called specificity. • No drug is truly specific but many have a relatively selective action on one type of receptor. • Drugs are prescribed to produce a therapeutic effect but they often produce additional unwanted effects which range from the trivial (slight nausea) to the fatal (aplastic anaemia)
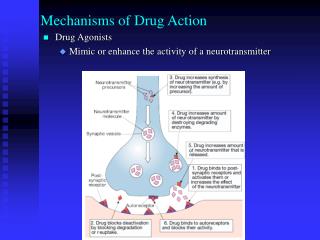
Neurotransmitters • Neurotransmitter substances are chemicals released from nerve terminals which diffuse across the synaptic cleft and bind to the receptors. • The neurotransmitter activates receptors, presumably by changing their conformation, and triggers a sequences of post-synaptic events resulting in, for example, muscle contraction or glandular secretion. • Following its release, the transmitter is inactivated by either degradation (e.g. acetylcholine) or reuptake (e.g. norepinephrine, GABA). • Many drugs act by either reducing or enhancing synaptic tranmission.
Hormones • Hormones are chemicals released into bloodstream; they produce their physiological effects on tissues possessing the necessary specific hormone receptors. • Drugs may interact with the endocrine system by inhibiting (e.g. antithyroid drugs) or increasing (e.g. oral antidiabetic agents) hormone release. • Other drugs interact with hormone receptors which may be activated (e.g. steroidal anti-inflammatory drugs) or blocked (e.g. oestrogen antagonists). • Local hormones (autacoids) such as histamine, serotonin (5-HT), kinins and prostaglandins are released in pathological processes.
Hormones • Propil tio urasil (PTU) obat antitiroid • Glimepirid dan glibenklamid, obat golongan sulfonilurea, digunakan untuk memacu skresi hormon insulin (abtidiabetik) • Efek dari histamin dapat dihambat oleh antihistamin • Beberapa obat dapat menghambat biosintesis prostaglandin (obat-obat anti inflamasi non-steroid, NSAIDs)
Neurotransmitter Asetilkholin Asetilkholin: • molekul pertama yang diidentifikasi sebagai neurotransmitter • aksinya pada sistem syaraf otonom di perifer maupun CNS • Di sistem syaraf perifer: • Neurotransmitter sistem syaraf parasimpatik (kholinergik) • memiliki 2 macam reseptor yaitu nikotinik dan muskarinik • Di sistem syaraf pusat (CNS): • berperan antara lain dalam regulasi belajar (learning), memori,kontrol gerakan, dan mood (perasaan) contoh: penyakit Alzheimer (pikun) disebabkan karena degenerasi sistim kolinergik
Reseptor kanal ion (ionotropik) • Teraktivasi sebagai respon terhadap ligan spesifik • Selektif terhadap ion tertentu • Terlibat dalam signaling sinaptik yang cepat (yang lambat : melalui reseptor protein G) • Contoh : reseptor asetilkolin nikotinik reseptor GABAa reseptor glutamat (NMDA) reseptor serotonin (5-HT3)
DRUG-receptor INTERACTION Kinetics, effect and fate
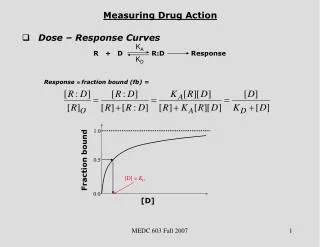
Kinetics…….. • A + R [AR] Response • Rate of association= k1 [A][R] • Rate of dissociation = k2 [AR] • At equilibrium: • Rate of association = rate of dissociation • k1 [A][R] = k2 [AR] • k2/k1 = [A][R]/ [AR] = kD
Kinetics…. (some assumptions) • 1.reaksi antara agonis dan reseptor adalah reversibel • 2. kedua reaktan tersedia dalam bentuk bebas atau terikat dan tidak termasuk bentuk lain, mis hasil degradasi yang tidak terlibat dalam reaksi tersebut • 3. Semua tempat di reseptor mempunyai affinitas yg sama terhadap agonis dan independen
Plot terhadap waktu…. • d([AR]/dt = k1[A][R] – k2[AR] • Plotting of [AR] as function of time yields an hyperbolic curve and asymptotic relationships for the formation of [AR] as equilibrium was approach
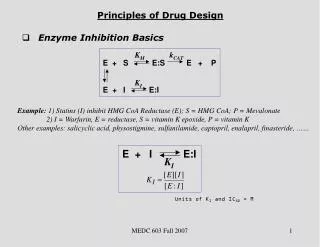
Type of antagonism • Competitive antagonism: atropine, ipratropium, hyoscine for ACTH-receptor • Irreversible antagonism: phenoxybenzamine for α-adrenoceptor • Non-competitive antagonism: Ca-channel blockers • Chemical antagonism: protamine vs heparin • Physiological antagonism: prostacyclin against thromboxane A2