Download
1 / 24
240 likes | 476 Views
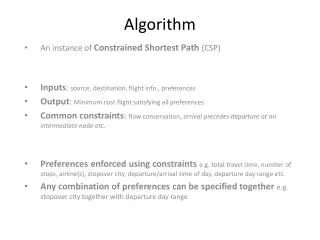
Algorithm. Dr. Patrice Junod Clinique m édicale l ’ Actuel. This activity is supported by an educational grant from:. 1- Algorithm Nephropathy Advisory Committee on the clinical management of people living with HIV 2- HIV and Renal Health – Management tool

E N D
Algorithm Dr. Patrice JunodClinique médicale l’Actuel This activity is supported by an educational grant from:
1- Algorithm Nephropathy Advisory Committee on the clinical management of people living with HIV 2- HIV and Renal Health – Management tool National Development Committee – Supported by Janssen Algorithm
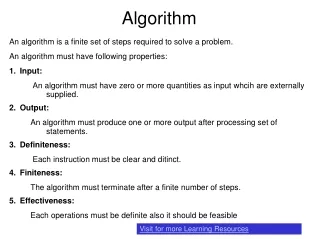
− Nephropathy − PERIODIC HEALTH EXAMINATION OF ADULTS LIVING WITH HIV (HUMAN IMMUNODEFICIENCY VIRUS) Advisory Committee on the Clinical Management of Persons Living with HIV
Screening for Kidney Problems Advisory Committee on the Clinical Management of Persons Living with HIV * Risk factors for CKD: Diabetes, hypertension, CVD, viral hepatitis, concomitant nephrotoxic drugs, family history of CKD, black African ethnicity
GFR using CKD-EPI or MDRD > 60 and < 90 cc/min < 60 cc/min* < 30 cc/min* Increase in Cr > 20% for > 3 months** Glucose+Protein+HypoPO4 ACRand MAU CaPO4 Renal ultrasound Refer to algorithms (next pages) Repeat CKD-EPI or MDRD calculation Refer to proteinuria algorithm (next page) Referral to nephrologist or internist GFR < 90 GFR > 90 * If GFR < 50 cc/min: consider adjusting the dose of certain ARV and concomitant medications ** Test for tubulopathy if GFR declines > 10 cc/min while on tenofovir Follow up every 3 months Regular follow-up
GFR using CKD-EPI or MDRD > 60 and < 90 cc/min < 60 cc/min* < 30 cc/min* Increase in Cr > 20% for > 3 months** Glucose+Protein+HypoPO4 ACRand MAU CaPO4 Renal ultrasound Refer to algorithms (next pages) Repeat CKD-EPI or MDRD calculation Refer to proteinuria algorithm (next page) Referral to nephrologist or internist GFR < 90 GFR > 90 * If GFR < 50 cc/min: consider adjusting the dose of certain ARV and concomitant medications ** Test for tubulopathy if GFR declines > 10 cc/min while on tenofovir Follow up every 3 months Regular follow-up
GFR using CKD-EPI or MDRD > 60 and < 90 cc/min Increase in Cr > 20% for > 3 months** Glucose+Protein+HypoPO4 Refer to algorithms (next pages) Repeat CKD-EPI or MDRD calculation * If GFR < 50 cc/min: consider adjusting the dose of certain ARV and concomitant medications ** Test for tubulopathy if GFR declines > 10 cc/min while on tenofovir GFR < 90 GFR > 90 Follow up every 3 months Regular follow-up
GFR using CKD-EPI or MDRD > 60 and < 90 cc/min < 60 cc/min* < 30 cc/min* Increase in Cr > 20% for > 3 months** Glucose+Protein+HypoPO4 ACRand MAU CaPO4 Renal ultrasound Refer to algorithms (next pages) Repeat CKD-EPI or MDRD calculation Refer to proteinuria algorithm (next page) Referral to nephrologist or internist GFR < 90 GFR > 90 * If GFR < 50 cc/min: consider adjusting the dose of certain ARV and concomitant medications ** Test for tubulopathy if GFR declines > 10 cc/min while on tenofovir Follow up every 3 months Regular follow-up
GFR using CKD-EPI or MDRD < 60 cc/min* < 30 cc/min* * If GFR < 50 cc/min: consider adjusting the dose of certain ARV and concomitant medications ** Test for tubulopathy if GFR declines > 10 cc/min while on tenofovir ACRand MAU CaPO4 Renal ultrasound Refer to proteinuria algorithm (next page) Referral to nephrologist or internist
Urinalysis or urine dipstick Glucose > 0 Protein ≥ 1 + or 0.25 g/L Fasting glucose + Rule out diabetes Repeat at next appt. Glycosuria DB + Glycosuria DB – Protein ≥ 1+ or 0.25 g/L Protein < 1+ or 0.25 g/L Repeat 1x ACR and MAU Normal DB follow-up ACR> 0.05 g/mmol or MAU > 2.1 mg/mmol or hematuria (> 2 RBC/HPF) ACR ≤ 0.05 g/mmol and MAU < 2.1 mg/mmol Glycosuria DB – • - Renal ultrasound • - Ascertain the risk factors • - Referral to nephrologist or internist, or to urologist for isolated hematuria Normal Referral to nephrologist or internist
Urinalysis or urine dipstick Glucose > 0 Protein ≥ 1 + or 0.25 g/L Repeat at next appt. Fasting glucose + Rule out diabetes Protein ≥ 1+ or 0.25 g/L Protein < 1+ or 0.25 g/L Glycosuria DB + Glycosuria DB – ACR and MAU Normal Repeat 1x DB follow-up ACR> 0.05 g/mmol or MAU > 2.1 mg/mmol or hematuria (> 2 RBC/HPF) ACR ≤ 0.05 g/mmol and MAU < 2.1 mg/mmol Glycosuria DB – • - Renal ultrasound • - Ascertain the risk factors • - Referral to nephrologist or internist, or to urologist for isolated hematuria Normal Referral to nephrologist or internist
Urinalysis or urine dipstick Glucose > 0 Fasting glucose + Rule out diabetes Glycosuria DB + Glycosuria DB – Repeat 1x DB follow-up Glycosuria DB – Referral to nephrologist or internist
Urinalysis or urine dipstick Protein ≥ 1 + or 0.25 g/L Glucose > 0 Fasting glucose + Rule out diabetes Repeat at next appt. Glycosuria DB + Glycosuria DB – Protein ≥ 1+ or 0.25 g/L Protein < 1+ or 0.25 g/L Repeat 1x ACR and MAU Normal DB follow-up ACR> 0.05 g/mmol or MAU > 2.1 mg/mmol or hematuria (> 2 RBC/HPF) ACR ≤ 0.05 g/mmol and MAU < 2.1 mg/mmol Glycosuria DB – • - Renal ultrasound • - Ascertain the risk factors • - Referral to nephrologist or internist, or to urologist for isolated hematuria Normal Referral to nephrologist or internist
Urinalysis or urine dipstick Protein ≥ 1 + or 0.25 g/L Repeat at next appt. Protein ≥ 1+ or 0.25 g/L Protein < 1+ or 0.25 g/L ACR and MAU Normal ACR> 0.05 g/mmol or MAU > 2.1 mg/mmol or hematuria (> 2 RBC/HPF) ACR ≤ 0.05 g/mmol and MAU < 2.1 mg/mmol • - Renal ultrasound • - Ascertain the risk factors • - Referral to nephrologist or internist, or to urologist for isolated hematuria Normal
Serum phosphorus < normal levels 0.65 – normal level Repeat in 3 months 0.32 – 0.65 mmol/L Repeat in 1 month Urinary fractional excretion of phosphorus if available (if > 20% or > 10% and hypophosphatemia: referral to a specialist Repeat and if < normal levels < 0.32 mmol/L Treat immediately Referral to nephrologist 25-OH Vit D PTH assay Albumin-corrected Ca < 50: deficiency < 75: insufficiency > 75 Abnormal Normal Abnormal Normal Vit D Rx Normal Referral to nephrologist or internist Referral to nephrologist or internist
Serum phosphorus < normal levels 0.65 – normal level Repeat in 3 months 0.32 – 0.65 mmol/L Repeat in 1 month Urinary fractional excretion of phosphorus if available (if > 20% or > 10% and hypophosphatemia: referral to a specialist Repeat and if < normal levels < 0.32 mmol/L Treat immediately Referral to nephrologist 25-OH Vit D PTH assay Albumin-corrected Ca < 50: deficiency < 75: insufficiency > 75 Abnormal Normal Abnormal Normal Vit D Rx Normal Referral to nephrologist or internist Referral to nephrologist or internist
Serum phosphorus < normal levels 0.65 – normal level Repeat in 3 months 0.32 – 0.65 mmol/L Repeat in 1 month Urinary fractional excretion of phosphorus if available (if > 20% or > 10% and hypophosphatemia: referral to a specialist Repeat and if < normal levels < 0.32 mmol/L Treat immediately Referral to nephrologist
Serum phosphorus < normal levels 0.65 – normal level Repeat in 3 months 0.32 – 0.65 mmol/L Repeat in 1 month Urinary fractional excretion of phosphorus if available (if > 20% or > 10% and hypophosphatemia: referral to a specialist Repeat and if < normal levels < 0.32 mmol/L Treat immediately Referral to nephrologist 25-OH Vit D PTH assay Albumin-corrected Ca < 50: deficiency < 75: insufficiency > 75 Abnormal Normal Abnormal Normal Vit D Rx Normal Referral to nephrologist or internist Referral to nephrologist or internist
Serum phosphorus < normal levels Urinary fractional excretion of phosphorus if available (if > 20% or > 10% and hypophosphatemia: referral to a specialist Repeat and if < normal levels 25-OH Vit D PTH assay Albumin-corrected Ca < 50: deficiency < 75: insufficiency > 75 Abnormal Normal Abnormal Normal Vit D Rx Normal Referral to nephrologist or internist Referral to nephrologist or internist