Download
1 / 21
391 likes | 2.05k Views
Late Sciences lecture series: Lecture 5. Fluid compartments and IV Fluid therapy. Mahesh Nirmalan Critical Care Unit, Central Manchester Foundation Trust & School of Bio Medicine University of Manchester, United Kingdom. Objectives. Distribution of water within the body

E N D
Late Sciences lecture series: Lecture 5 Fluid compartments and IV Fluid therapy Mahesh Nirmalan Critical Care Unit, Central Manchester Foundation Trust & School of Bio Medicine University of Manchester, United Kingdom
Objectives • Distribution of water within the body • Distribution of electrolytes • Principles of IV fluid therapy • Common IV fluids
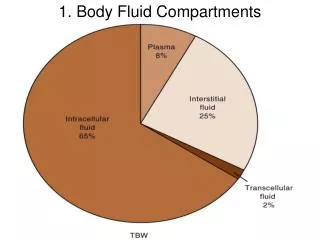
5% COP ECF 20% of body weight Osmolality 15% ICF = 40% of body weight Fluid compartments 60-70% of total body weight is made up of water
Exchange of fluid between capillaries and tissues COP=20 mm • Oedema formation • Definition of generalised oedema • Definition of localised oedema 32 mm 12 mm
Fluid spaces • 1st Spacing: Normal distribution within ECF and ICF • 2nd spacing: accumulation within the interstitial compartments: oedema formation but available for physiological exchange between compartments • 3rd spacing: Accumulation in parts of the body where it’s not available for exchange between the different compartments: Ascitis, tissue inflammation, oedema from burns/surgery
Greater number of osmotically active particles Composition of body fluids Na,K ATPase • Na+, Cl-, HCO3- are predominantly in the ECF • K+, Mg2+, PO43- are predominantly in the ICF • The electrolyte composition of plasma and interstitial fluids are broadly similar • The main difference between plasma and interstitial fluid is the high protein content in the plasma • All compartments are electrically neutral • More cations (>2%) in the plasma due to the “Donnan effect”: ??? • Slightly more anions in the interstitial fluid • Change in plasma proteins have important effects on cell functions that are poorly understood • Malnutrition, Nephrotic syndrome, critical illness
The distribution of fluid between the ICF and ECF compartments is mainly determined by the osmotic effects of the small inorganic ions: Na+, Cl- If the osmotic properties of the ECF is constant there will be minimal fluid shifts between the ICF and ECF
Changes in free water content will alter the osmotic effects Plasma 5% Interstitium 25% Distribution of free water • General increase or decrease in total body water will involve all the 3 fluid compartments • Most of the quantitative effects will be “buffered” by the ICF • Hypotension is a very late sign of dehydration • If free water is administered most of the administered volume will reach the ICF with very little change in plasma volume • Distribution ratio of free water ICF 70% In the absence of loss of ECF (vomiting diarrhoea etc) changes in Na+ is usually the result of changes in free water content
1 liter 5% Dextrose Total body water=1 liter ECF=1/3 ~ 350ml ICF=2/3 ~ 650ml Intravascular ~1/5 of ECF~70ml
Fluid distribution within the ECF • The ECF has a uniform electrolyte composition • Distribution of fluid between the interstitium and plasma is determined by plasma proteins and the COP • Isotonic fluids will dilute plasma proteins and reduce COP • Isotonic fluids will distribute between the interstitial fluid compartment and plasma • Distribution ratio of a litre of isotonic fluid Plasma 33% Interstitium 66%
1 Litre 0.9% saline Total body water ICF=0 ECF=1 litre Interstitial=2/3 of ECF=650ml Intravascular =1/3 ECF=350 ml
1 liter 5% Albumin Intravascular=1 liter
How much? What? • Current deficits • Anticipated maintenance requirements: 1ml/kg/hr • Ongoing losses: urine, evaporation, drainage • Abnormal increase in basal requirements • Anticipated fluid shifts Which compartment are we trying to replenish Total fluids Plasma Plasma substitutes ECF losses 5% Dextrose Isotonic crystalloids IV Fluids
Dehydration Current Deficits Hypernatraemia is a very common feature of free water loss Mild C/O Thirst But no clinical signs of dehydration Up to 5% deficit in TBW Will affect all fluid compartments Severe Cardiovascular signs Tachycardia /hypotension Marked peripheral signs of dehydration >15% of TBW Moderate Objective clinical signs of dehydration Mucous membranes, skin turgor, mild tachycardia Reduced UOP 5-15% of TBW
IV Fluids • 5% Dextrose: Free water • Dextrose saline • Commonest cause for hyponatraemia in the surgical population • The myth of 3:1 • Crystalloids: 0.9% NaCl, RLS • N.saline (150 mmol Na+ and 150 mMol Cl-) • Not very physiological • Hyperchloraemic acidosis…….Why? • Colloids: Gelatin based, starch based, albumin • Blood and blood products
Ringer’s Lactate solution • Na+: 130mMol/l • Cl-: 109mMol/l • Lactate: 28mMol/l • K+: 4mMol/l • Ca2+: 3mEq/l
Case study • Elderly male; Height: 5 feet 11 inches • Weight: 52Kg • H/O duodenal ulcer • Abdominal pain • Severe vomiting of 3 weeks duration • Unable to retain any food or drinks • Wasted, dehydrated DD??
Pyloric stenosis • What is the extent of dehydration would you expect in this patient? • What would be the clinical signs? • What electrolyte changes would you expect? • How much fluid? • What fluid? • Over what period?
22 years old university student65 KgLife long Lib Dem supporterFeels betrayed by the formation of the new “Libservative” government72 hours of hunger strike opposite the LibDem HQ • What would the fluid deficit be? • Serum electrolytes? • What is the replacement fluid? • Over how long?
72 years old female • Radical hysterectomy in the morning • 2 litres blood loss • 2 litres blood transfused • 5% dextrose infusion: 75ml/hr • Called at 2 AM to review as she has not passed urine for the past 5 hours • Conscious, cold and clammy • pH 7.31; BE -9; lactate 2.2; Hb: 14.3 • Pulse 122/min; BP 70/45; RR 18/min