Download
1 / 16
170 likes | 193 Views
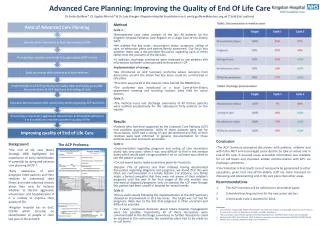
Explore quality improvement in healthcare systems, addressing underuse, misuse, and overuse issues to enhance patient outcomes and satisfaction. Learn about strategies, indicators, and policy changes. Stay informed on the latest advancements in patient safety and quality benchmarks.

E N D
ImprovingQuality of Care Systems Grant T. Savage, PhD Eric S. Williams, PhD UAB-Tuscaloosa
What is Health Care Quality --And How Can We Measure It? • Structures – facilities, personnel, technologies, etc. • Processes – the provision of care services; use of structural resources • Outcomes – results from the production of care Source: Donabedian (1966)
What is Quality in Practical Terms? • Patient Satisfaction • Relationships: Information and Emotional Support • Decision-making Efficiency • Patient Outcomes • Amenities and Convenience Source: Chilingerian (2004)
What are Quality Problems? • Underuse – failure to provide a service whose benefit is greater than its risk • Misuse – right service is provided poorly, and an avoidable complication reduces benefit to patient • Overuse – health services provided when its risk outweighs its benefit Source: Chassin (1997)
Underuse • Many proven, effective interventions are available, but not widely used: • Beta-blockers for heart attack patients (21% of eligible elderly patients) • Clinical detection of depression • Recommending mammograms, pap smears • Diabetic eye and foot exams • Resistance to clinical guidelines as “cookbook medicine” Source: Chassin (1997)
Overuse • Many unnecessary or inappropriate services • RAND study of inappropriate use: • 17% coronary angiographies • 32% of carotid endarterectomies • 17% of upper gastrointestinal endoscopies • 7-51% of sedatives, hypnotics, antidepressives, and antipsychotics are overused with elderly patients • Use of objective standards revealed between 10-27% of procedures are inappropriate Source: Chassin (1997)
Misuse • Higher rates of morbidity and mortality of surgery patients in low volume hospitals • Medication errors • Medical errors • Adverse events Sources: Chassin (1997); Kohn, Corrigan & Donaldson (2000); Committee on Quality Health Care in America, IOM (2001)
What Causes the Quality Chasm? • Fragmented and decentralized system of care creates quality deficits for patients • Inadequate attention within licensing and accreditation processes to medical errors • Medical liability inhibits physicians from reporting errors and improving processes • Third party payers provide no incentives to providers to increase patient safety Source:Bleich (2005)
What Causes the Quality Chasm? • Consumers are unable to perceive quality differences among health care services • Benefits from quality improvement often are displaced in time and space • Administrative pricing prevents consumers and third-party payers from paying for quality • Clinicians do not have access to information about best practices Sources: Newhouse (2002); Blumenthal & Ferris (2004)
What Causes the Quality Chasm? • Ways of changing provider behavior are not well understood • Primitive science of quality measurement • Inadequate health care system infrastructure (e.g., IT) • Major legal obstacles • Government financial difficulties Source:Blumenthal & Ferris (2004)
Past Approaches to QI • Regulation • Government – CMS, FDA, etc. • Accreditation – JCAHO, NCQA, etc. • Competition • Management - CQI • Financial Incentives Source: Chassin (1997)
QI: Tactical & Strategic Levels • Tactical/operational level • Level A – experience of patients and communities • Level B – microsystems of care • Strategic/policy level • Level C – health care organizations • Level D – health care environment Source: Berwick (2002)
Strategic QI for the Public Sector • Government should increase R&D to: • Understand processes of care that impact quality • Improve and extend quality measures • Understand how pay-for-performance affects quality • Develop standards for IT system data interoperability • Government should: • Help develop a national health information infrastructure • In the U.S., remove legal restrictions.: • On contracting for quality and using gain-sharing to reward performance • That inhibit physician-hospital IT-based alliances Source: Blumenthal & Ferris (2004)
Patient Safety Center at AHRQ Developed centers of excellence in patient safety research Developed three sets of Quality Indicators for hospitals and providers Error Reporting System 22 states now have mandatory reporting of medical errors (up from 15 in 2000) Controversy: What counts as an adverse event? Bleich (2005) QI: What’s Been Done in the U.S.
QI: What’s Been Done Recently • Performance Standards • JCAHO has introduced accreditation standards in patient safety that include root cause analysis of adverse events • AHRQ has conducted research to measure the incident of adverse events and to develop benchmarks for improvement • Leapfrog Group has tried to tie quality improvement efforts by providers to contracts with large employers • Safety Systems within Health Care Organizations • Focus mostly on medication errors • Computer-based Physician Order Entry (CPOE) • Assessments of medication processes • VA voluntary, non-punitive Patient Error Reporting System Bleich (2005)
References Berwick, D. M. (2002). A user's manual for the IOM's 'Quality Chasm' report. Health Affairs, 21(3), 80-90. Bleich, S. (2005). Medical errors: Five years after the IOM report (Issue Brief). New York: The Commonwealth Fund. Blumenthal, D., & Ferris, T. (2004). The business case for quality: Ending business as usual in American health care. New York: The Commonwealth Fund. Chilingerian, J. (2004). Who has star quality? In R. E. Herzlinger (Ed.), Consumer-driven health care: implications for providers, payers and policy makers (pp. 443-453). San Francisco: Jossey-Bass. Committee on Quality Health Care in America, IOM. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press. Donabedian, A. (1966). Evaluating the quality of medical care. Milbank Memorial Fund Quarterly, 44(3), Suppl:166-206. Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To err is human: Building a safer health system. Washington, DC: National Academy Press. Newhouse, J. P. (2002). Why is there a quality chasm? Health Affairs, 21(4), 13-25.