Download

1 / 37
400 likes | 952 Views
EXTENSOR TENDON INJURIES. EXTENSOR TENDON INJURIES. EXTENSOR TENDONS ARE PREDISPOSED TO LACERATION 1. DUE TO SUPERFICIAL LOCATION ON DORSUM OF HAND 2. MINIMAL AMOUNT OF SUBCUT. TISSUE BETWEEN TENDONS AND OVERLYING SKIN RESULTS OF TREATMENT ARE NOT ALWAYS AS

E N D
EXTENSOR TENDON INJURIES • EXTENSOR TENDONS ARE PREDISPOSED TO LACERATION 1. DUE TO SUPERFICIAL LOCATION ON DORSUM OF HAND 2. MINIMAL AMOUNT OF SUBCUT. TISSUE BETWEEN TENDONS AND OVERLYING SKIN • RESULTS OF TREATMENT ARE NOT ALWAYS AS FAVORABLE AS ONCE ASSUMED
ANATOMY • EXTENSOR TENDON ON THE DORSUM OF THE HAND TO THE LEVEL OF THE MCPJ ARE COMPOSED OF MUSCULOTENDINOUS UNITS • TENDONS RADIAL ===> ULNAR EPB,EPL,EIP,EDC,EDQM • GAIN ACCESS BY PASSING THROUGH FIBRO-OSSEOUS TUNNELS AT THE WRIST LEVEL, AND AT THIS LEVEL ARE COVERED BY TENOSYNOVIUM
ANATOMY • NEAR THE MIDPORTION OF THE METACARPALS, JUNCTURA TENDINUM PASS DISTALLY AND OBLIQUELY BETWEEN THE ULNAR THREE EDC TENDONS • COMPARTMENTS PREVENT EXT. TENDONS FROM BOWSTRINGING DORSALLY DURING ACTIVE FINGER EXTESION, PARTICULLARLY WHEN WRIST IS EXTENDED • JUNCTURA RESULT IN GROUPED EDC EXTENSION, ESPECIALLY AT THE ULNAR ASPECT OF THE HAND
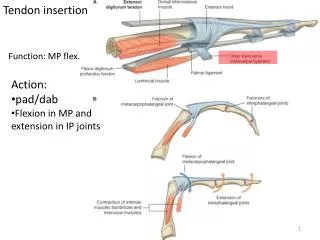
ANATOMY • AT THE MPJ LEVEL THE EIP AND EDC TO THE INDEX JOIN TOGETHER THE TENDONS AND ARE CENTRALIZED OVER THE DORSUM OF THE MPJ BY SAGITAL BANDS • TRANSVERSE FIBERS CONNECT THE LATERAL MARGINS OF THE EXT TENDONS TO THE PALMAR PLATES OF THE MPJ AND TO THE PERIOSTEUM OF THE PROXIMAL PHALLYNX • DISTAL TO THE SAGITTAL BANDS ARE TRANSVERSE AND OBLIQUE FIBERS===>INITIAL CONTRIBUTIONS OF THE INTEROSSEOUS MM TO THE DORSAL APPARATUS
ANATOMY • DISTAL TO THE MPJ THE DIGITAL EXTENSOR MECHANISM CONSISTS OF BOTH INTRINSIC AND EXTRINSIC MUSCULOTENDINOUS UNITS • AT THE MPJ LEVEL ALL COMPONENTS OF INTRINISIC MUSCLES ARE PALMAR TO THE AXIS OF ROTATION AND SERVE AS MPJ FLEXORS • DISTAL TO THE MPJ EXTRINSIC AND INTRINSIC TENDONS JOIN TOGETHER FORMING THE DORSAL APPARATUS • CONTINUATION OF THE EXTRINSIC EXTENSOR IS THE CENRAL SLIP WHICH INSERTS ON THE BASE OF THE MIDDLE PHALLYNX
ANATOMY • INTRINSIC TENDONS FORM THE LATERAL BANDS WHICH SEND FIBERS MEDIALLY TO FORM PART OF THE CENTRAL SLIP • LATERAL BANDS JOIN ON THE DORSUM OF THE MIDDLE PHALLYNX FORMING THE CONJOIN TENDON AND INSERTS ON THE BASE OF THE DISTAL PHALLYNX
OPEN INJURIESDISTAL FOREARM AND WRIST (ZONE 8 & 7) • DEEP LACERATIONS USUAL CAUSE AT THIS LEVEL • TENDONS MAY RETRACT WELL PROXIMAL INTO THE FOREARM • LACERATIONS OF THE SUPERFICIAL RADIAL BRANCHES AND LATERAL ANTEBRACHIAL CUTANEOUS NERVES ARE COMMONLY ASSOC. • SURGICAL APPROACH REQUIRES LONGITUDINAL EXPOSURE • 4-0 NONABSORBABLE SUTURE WITH KNOTS BURIED
DISTAL FOREARM AND WRISTZONE 8 & 7 CONT. • SPECIFIC PROBLEMS OCCUR AT THE LEVEL OF THE EXTENSOR RETINACULUM 1. COMPARTMENTS ARE WELL DEFINED BY A RETINACULUM AND SEPTA BOTH OF WHICH APPROXIMATE TENDONS CLOSELY 2. COMPARTMENTS MAY HAVE TO BE OPENED, OR A PORTION EXCISED TO RETRIEVE RETRACTED ENDS AND ACCOMMODATE BULK OF TENDON REPAIR
OPEN INJURIESZONE 8 & 7 POST-OP CARE • WRIST SPLINTED 20 DEGREES EXT. AND MP JOINTS NEUTAL 10 DAYS • SPLINT CHANGED TO ALLOW MPJ 30-40 DEGREES 4 WEEKS • SPLINT REMOVED TO BEGIN PROTECTED AROM UNTIL 6 WEEKS POST-OP • MULTIPLE TENDON INJURIES: 1. DYNAMIC EXTENSION SPLINTING AS SOON AS LOCAL WOUND PERMITS. 2. STATIC HAND AND WRIST SPLINT 4 WEEKS AFTER SURGERY 3. PERIODIC REMOVAL WITH AROM 6 WEEKS P/O
OPEN INJURIESZONE 6 • TENDONS VERY SUPERFICIAL • ASSOC INJURIES WITH PARATENON AND PERIOSTEUM RESULT IN INC. ADHESIONS • ASSCO LACS OF BRANCHES OF SUP RADIAL AND DORSAL ULNAR N. • TENDONS ARE ROUND OR OVAL AND WILL ACCEPT KESSLER STITCH, 4-0 NONABSORBABLE
OPEN INJURIESZONE 6 POST OP • STATIC SPLINT WRIST 30 DEG EXT, MP NEUTRAL 10 DAYS • SPLINT CHANGE AT 10 DAYS, FLEXING MPJ AT 30 DEGREES • 4 WEEKS PERIODIC REMOVAL OF SPLINT, AROM • D/C SPLINT AT 6 WEEKS • SPLINT ALL THREE ULNAR DIGITS IF ONE OR MORE INJURED, IF & THUMB TREATED INDEP.
OPEN INJURIESMETACARPOPHALANGEAL JOINT LEVEL (ZONE 5) • LACERATIONS READILY ENTER THE JOINT • MUST CONSIDER HUMAN BITE AT THIS LEVEL • RADIOGRAPHS TO ASSESS METACARPAL HEAD ARE ESSENTIAL • OPEN JOINT INJURIES SECONDARY TO HUMAN BITES REQUIRE THOROUGH DEBRIDEMENT AND PARENTERAL ANTIBIOTICS • TENDON ENDS DO NOT RETRACT AT THIS LEVEL • LACERATION MAY BE PROXIMAL TO SKIN LAC DUE TO FLEXED MPJ
OPEN INJURIESMETACARPOPHALANGEAL JOINT LEVEL (ZONE 5) • LACERATIONS READILY ENTER THE JOINT • MUST CONSIDER HUMAN BITE AT THIS LEVEL • RADIOGRAPHS TO ASSESS METACARPAL HEAD ARE ESSENTIAL • OPEN JOINT INJURIES SECONDARY TO HUMAN BITES REQUIRE THOROUGH DEBRIDEMENT AND PARENTERAL ANTIBIOTICS • TENDON ENDS DO NOT RETRACT AT THIS LEVEL • LACERATION MAY BE PROXIMAL TO SKIN LAC DUE TO FLEXED MPJ
OPEN INJURIESMETACARPOPHALANGEAL JOINT LEVEL (ZONE 5) • LACERATIONS READILY ENTER THE JOINT • MUST CONSIDER HUMAN BITE AT THIS LEVEL • RADIOGRAPHS TO ASSESS METACARPAL HEAD ARE ESSENTIAL • OPEN JOINT INJURIES SECONDARY TO HUMAN BITES REQUIRE THOROUGH DEBRIDEMENT AND PARENTERAL ANTIBIOTICS • TENDON ENDS DO NOT RETRACT AT THIS LEVEL • LACERATION MAY BE PROXIMAL TO SKIN LAC DUE TO FLEXED MPJ
OPEN LACERATIONSMETACARPOPHALANGEAL JOINT ZONE 5 • OBLIQUE LACERATIONS MAY INCLUDE SAGITTAL BANDS, SHOULD BE CAREFULLY SUTURED TO PREVENT LATERAL MIGARATION OF THE EDC • SIMPLE LACERATIONS WHICH EXTEND INTO JT. 1. CAREFUL INSPECTION AND I&D OF JOINT CLOSURE AS SEPARATE LAYTER 4-0 ABSORBABLE SUTURE 2. JOINT CONTAMINATED: PORTION OF CAPSULE EXCISED AND LEFT OPEN, WICK 48HRS, IV ABX
OPEN INJURIESZONES 3 & 4 PIP JOINT LEVEL • DORSAL APPARATUS THIS AND CIRCUMFERENTIALLY ORIENTED • SIMPLE LACERATIONS SELDOM RESULT IN COMPLETE LACERATIONS OF DORSAL APP. • ENDS DO NOT RETRACT • SIMPLE INJURIES RE-APPROX WITH 5-0 NONABS • IF PARTIAL SUBSTANCE LOSS OF DORSAL APP. 1. BETTER TO ALLOW REMAINING TENDON TO ASSUME NORMAL RESTING TENSION THAN TO APPROX. UNDER TENSION
OPEN LACERATIONSPIPJ LEVEL ZONES 4 & 3 • LACERATIONS DISTALLY INTO ZONE 3 MAY EXTEND INTO PIPJ • ZONE 3 LACERATIONS OCCUR WHERE THE EXTENSORS AND LATERAL BANDS COMBINE TO FORM THE CENTRAL SLIP • OPEN INJURIES OF THE CENTRAL SLIP MAY CAUSE ACUTE BOUTONIERE DEFORMITY • PROGRESSION TO ADVANCED BOUTONNIERE DEFORMITY SHOULD NOT BE UNDERESTIMATED • EXPLORATION OF CENTRAL SLIP IS MANDATORY • PROTECTIVE SPLINTING ADVISED
OPEN LACERATIONSZONE 4 & 5 • PARTIAL OR COMPLETE SIMPLE LACERATIONS, REPAIR WITH 5-0 NONABS. FIG-8 WITH NOT BURIED • IF DISTAL STUMP TOO SMALL TO ACCEPT SUTURE==> ATTATCH PROXIMAL CENTRAL SLIP DIRECTLY TO DORSAL FLARE OF MIDDLE PHALANX WITH T-VERSE DRILL HOLES • IF EXT. TENDON LAC EXTENSIVE PRECLUDING DIRECT REPAIR, MAY RECONSTRUCT USING PORTION OF THE LATERAL BANDS
OPEN LACERATIONSZONE 4 & 3 • PIVOTAL POINT IN REHAB FOR ZONE 4 & 3 INJURIES IS PREVENTION OF EARLY PIP FLEXION POSTURE • INCREASED TENSION IN THE REPAIRS AND PALMAR MIGRATION OF THE LATERAL BANDS MUST BE AVOIDED ==> WILL OCCUR IF PIPJ IS ALLOWED TO FLEX • COMPLEX INJURIES/NONCOMPLIANT PATIENT MAY REQUIRE K-WIRES TO TRANSFIX PIPJ IN EXTENSION
OPEN LACERATIONSZONE 4 & 3 • K-WIRES NEED TO BE REMOVED 3 WEEKS • EXTERNAL SPLINTING ADDITIONAL 3-4 WEEKS • RUBBER-BAND OR SPRING LOADED REVERSE KNUCKLE BENDERS ARE USED TO MAINTAIN EXTENSION WHILE ALLOWING ACTIVE FLEXION EXERCISES AFTER TOTAL OF 6 WEEKS INTERNAL/EXTERNAL STATIC SPLINTING • ALL SPLINTING IS DISCONTINUED AT 8 WEEKS • IF PLASTER SPLINTING: WRIST EXT 30 DEG. MP FLEXED 30 DEG. AND PIPJ IS IN NEUTRAL
OPEN INJURIESMIDDLE PHALANGEAL AND DIPJZONES 2 & 1 • LATERAL BANDS BLEND DORSALLY TO FORM THE CONJOINT TENDON, THEY ARE THIN AND ORIENTED AROUND THE DORSAL HALF OF THE MIDDLE PHALLYNX • SIMPLE LACS SELDOM TRANSECT ALL DORSAL APP. • READILY APPROX. WITH FIG. 8 NONABSORB. SUT. • IF SEGMENTAL LOSS OF PART OF THE APPARATUS IT MAY BE BETTER TO ALLOW REMAINING INTACT TENDON TO ASSUME NORMAL RESTING TENSION
OPEN INJURIESMID PHALANGEAL AND DIPJ • ZONE 1: CONJOINT TENDON IS WELL DEFINED AND DORSALLY POSITIONED • COMPLEX LACS WILL RESULT IN FLEXED DIPJ 40 DEG. • INCOMPLETE LACS ==> FLEXED DIPJ 15 DEG. AND EXT. WEAKNESS • REPAIRED WITH FIG 8 NONABS. 1. SEPARATE LAYER CLOSURE 2. RUNNING STITCH WITH BOTH SKIN & TENDON
ZONE 1 AND 2 REHAB • CONTINUOUS SPLINTING WITHOUT EXCEPTION IN FULL EXTENSION FOR 6 WEEKS • PROTECTED AROM EXERCISES AFTER SPLINT REMOVAL • NONCOMPLIANT PATIENTS : 0.O45 K-WIRE FOR 6 WEEKS, FOLLOWED BY PROTECTED, AROM FOR 2 WEEKS
CLOSED INJURIES • CENTRAL SLIP AND THE CONJOINT TENDON INSERT INTO THE DORSAL BONY PROMINENCES OF THE MIDDLE AND DISTAL PHALANGES • DIRECT, DEEP CONTUSIONS OR JOINT INJURIES MAY AVULSE THESE TENDONS AT THEIR INSERTIONS • CENTRAL SLIP INJURED: CLOSED BOUTONNIERE DEFORMITY • CONJOINT TENDON INJURED: CLOSED MALLET DEFORMITY • OFTEN MISSED OR UNDERTREATED
BOUTONNIERE DEFORMITY • THREE MECHANISMS OF INJURY TO PIPJOINT WILL RESULT IN DISRUPTION OF THE CENTRAL SLIP 1. DEEP CONTUSION ABOUT DORSUM OF PIPJ 2. ACUTE FORCEFUL FLEXION OF PIPJ 3. PALMAR DISLOCATION OF PIPJ • THESE INJURIES RESULT NOT ONLY IN CENTRAL SLIP DISRUPTION BUT PALMAR MIGRATION OF THE LATERAL BANDS • PULL OF INTRINSICS ARE FOCUSED ON THE DIPJ CAUSING DIPJ HYPEREXTENSION
BOUTONNIERE DEFORMITY • OFTEN NOT APPARENT FOR 7-14 DAYS • INITIALLY ASSOC WITH PAINFUL SWOLLEN PIPJ • EARLY FINDINGS 1. PAINFUL SWOLLEN PIPJ 2. MILD EXTENSION LAG (15-25 DEGREES) 3. DECREASED EXTENSION AGAINST RESISTANCE
BOUTONNIERE TREATMENT • KEY : MAINTAINING PIPJ IN CONSTANT COMPLETE EXTTENSION • POSITIONING DOES NOT REQUIRE SPLINTING DIP OR MPJ IN ANY SPECIFIC POSISTION • CONTINUOUS SPLINTING 6 WEEKS • IF ANY EVIDENCE OF RECURRANCE OF EXT LAG. ==> CONT. SPLINTING TOTAL OF 8 WEEKS • MAY OCCURE WITH AVULSION OF DORSAL LIP OF MIDDLE PHALLYNX, REQUIRES OPEN TREATMENT
MALLET DEFORMITY • USUALLY OCCURS WHEN TIP OF FINGER IS STRUCK BY OR AGAINST AN OBJECT RESULTING IN ACUTE FLEXION AT DIPJ • MAY \MAY NOT OCCUR WITH AVULSION OF SMALL FRAGMENTS OF BONE • NONOPERATIVE TREATMENT MOST WIDELY USED • GOAL OF TREATMENT IS MAINTENANCE OF CONTINUOUS DIPJ EXTENSION UNTIL TENDON HEALS
MALLET DEFORMITY TREATMENT • IN COOPERATIVE PATIENT: 1. CONTINUOUS SPLINTING FOR 6 WEEKS 2. FOLLOWED BY 2 WEEKS OF NIGHT SPLINTING 3. SPLINTING MUST BE RESUMED IF EVIDENCE OF RECURRENT EXTENSION LAG 4. OPEN CONJOINT TENDON INJURIES: TRANSFIXING DIPJ WITH 0.045 K WIRES FOR 6 WEEKS
MALLET FINGER TREATMENT • SMALL DORSAL AVULSION FRAGMENTS 1. DO NOT CONFUSE WITH HYPEREXTENSION INJURIES OF THE DIP WITH LARGE DORSAL FRAGMENTS, ASSOC WITH PALMAR SUBLUXTION OF DISTAL PHALANX **TREATMENT OF SMALL DORSAL AVULSIONS RESULTING FROM HYPERFLEXION WITH EXT SPLINTING IS NONCONTROVERSIAL **LARGE FX FRAGMENT FROM HYPEREXTENSION: TREATMENT SOMEWHAT CONTROVERSIAL. MOST COMMONLY TREATED WITH ORIF
INJURY ZONE AND OUTCOME RELATIONSHIP • ZONE 6 ( BACK OF HAND) KELLY NOTED NO POOR RESULTS • 20% POOR RESULTS AT LEVEL OF EXTENSOR RETINACULUM AND OVER DORSUM OF THE FINGERS • ZONE 7 INJURIES AT EXTENSOR RETINACULUM HAVE IMPROVED • ZONE 3 &4 (PROXIMAL PHALANX AND PIPJ) HAVE REMAINED PROBLEMATIC
CONCLUSION • FUNCTIONAL OUTCOMES AFTER EXTENSOR TENDON INJURIES HAVE RECEIVED LIMITED ATTENTION • PTS AS A GROUP WITH THIS INURY GENERALLY EXPERIENCE DECREASE GRIP STRENGTH OF 95% UNAFFECTED HAND • APPROX. 95% PATIENTS EXPRESS SATISFACTION