Download
1 / 35
450 likes | 1.03k Views
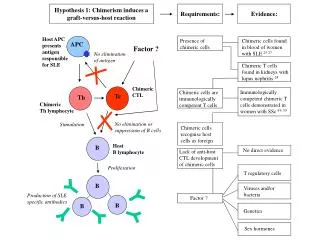
Graft vs. Host Disease. What is GVHD?. An cell mediated reaction of donor origin against recipient tissues It requires: a donor graft with immunologically competent cells a recipient unable to mount immune response recipient expresses tissue antigens that are not present in the donor.

E N D
What is GVHD? • An cell mediated reaction of donor origin against recipient tissues • It requires: • a donor graft with immunologically competent cells • a recipient unable to mount immune response • recipient expresses tissue antigens that are not present in the donor.
Risk Factors Age HLA mismatch CMV positive multiparous female male Tissue injury Signs/Symptoms Liver Cholestasis Skin inflammatory rash Gut Secretory diarrhea Clinical Features of Acute GVHD
Very Basic Immunology • Auditors - responsible for sifting thru all available info to find evidence of intrusion. Shows data to Regulators and Enforcers. • Regulators - Reviews data presented by Auditor and contacts Enforcers. (includes prosecutors and defenders) • Enforcers - Kill things.
Dendritic cells B cells Macrophages Endothelial Cells Kupffer cells Sample Outside Sample Inside Process Specimen Present Data Auditors
Auditor (Sampling surroundings) Degraded in peptides Combined with HLA molecules Exogenous substance Displayed with HLA molecule
Auditor (Sampling inside) Viral or intracellular protein Nucleus Virus Displayed with HLA molecule
Communicating Trouble HLA Class II - i.e. HLA - DR, DQ, DP “Regulator” “Trouble” signal CD4 Dendritic cell B cell Macrophage “Meaning of Life” “Enforcer” CD8 HLA Class I - i.e. HLA-A, B, C
Why do we have to match? • BMT = immune system transplant • HLA molecules act as T cell “superantigens” • All somatic tissues express HLA class I • Transferred T cell could “over-react” • Transferred T cells won’t work if they can’t bind their own HLA molecule
If there is a “match”, why GVHD? • HLA molecules “show” what’s inside • We are all different inside • GVHD results from T cell reactivity toward polymorphisms between donor and host. • This can be a good thing • or • This can be a bad thing
H -Y antigen from Y chromosome expressed ubiquitously target for CTL responses CTL response leads to less relapse, more GVHD HA-1 polymorphic unknown function expressed only on hematopoietic cells target for CTL responses CTL response leads to less relapse, no GVHD Polymorphisms can help rid disease or cause GVHD
GVHD Prophylaxis - How much? • Aggressive Prophylaxis • LESS GVHD • MORE infection • MORE relapse • Minimal Prophylaxis • MORE GVHD • LESS infection • LESS relapse SURVIVAL
Graft vs. Lymphoma Juckett, et al BMT 21:893, 1998
Myeloablative SCT High dose chemo High dose radiation Stem cells Watch and wait
Non-myeloablative SCT Stem cells Immuno suppression Manipulate the Immune response to maximize G vs. disease
Infection after SCT • Infection is the most common cause of non-relapse death • Risk increases with: • previous treatment • history of infection (especially fungal) • tissue injury (especially mucositis) • duration of neutropenia • GVHD and treatment thereof (prednisone) • mismatched/unrelated vs. matched/related
Infection of SCT patientsPhase I - first month • Host immune system defect • skin, mucous membrane, neutropenia • Pathogens • staph epidermidis • facultative gram neg bacilli • oropharyngeal streptococci • all candida, aspergillus • respiratory and enteric viruses
Infection of SCT patientsPhase II - 30 to 100 days • Host immune system defect • Impaired cellular immunity, GVHD • Pathogens • CMV • all candida, aspergillus • staph epidermidis • respiratory and enteric viruses • EBV (for T cell depleted SCT)
Infection of SCT patientsPhase III - > 100 days • Host immune system defect • Impaired cellular and humoral immunity • Pathogens • CMV • Encapsulated bacteria • Aspergillus species • varicella-zoster, EBV • PCP, Toxoplasma
Incidence 10 - 20% Mortality 70% Autopsy 10 - 30% Candidasp. Krusei, glabrata Aspergillus sp. Diagnosis difficult Invasive Fungal Infection
Strong Association Acute GVHD ATG treatment Age Fungal colonization Long neutropenia Dx: AML HLA mismatched Weak Association Splenectormy CMV Pos TBI low BM dose HSV positive donor Risk Factors for Invasive Fungal Infection
Available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr4910a1.htm
Systemic Fungal Infections Diagnosed in HSCT Recipients, by Prophylaxis Used YesNoTotal Fluconazole 5 (3%) 174 179 Placebo 28 (16%) 149 177 Total 33 323 356 OR = 0.15, 95% C.I. (0.05, 0.42), P < 0.001 Goodman JL, et al. N Engl J Med 1992;326(13):845-851.
Allogeneic HSCT recipients • Rooms with >12 air exchanges/hour [AIII] • Point-of-use high efficiency (>99%) particulate air (HEPA) filters that are capable of removing particles >0.3 µm in diameter [AIII] Autologous HSCT recipients • Use of HEPA-filtered rooms should be considered for autologous HSCT recipients if they develop prolonged neutropenia [CIII] Ventilation Recommendations
Positive Room Air Pressure • Hospital rooms for HSCT recipients should have positive room air pressure • HSCT units should maintain consistent pressure differentials between the patient’s room and the hallway or anteroom at >2.5 Pascals or 0.01 inch by water gauge [BIII]
Equipment and Supplies • All HSCT units should sterilize or disinfect and maintain equipment and devices using only FDA-or EPA-registered compounds as directed by established guidelines [AIII] • HSCT units should monitor opened and unopened wound dressing supplies [BIII] • Monitoring should consist of discarding all bandages and wound dressings that are out of date, have damaged packaging, or are visually contaminated by construction debris or moisture [BIII]
NO • Routine bacterial and fungal patient surveillance cultures [DII] YES • Routine fungal environmental surveillance cultures [CIII] • Routine surveillance for the number of aspergillosis cases in HSCT recipients [BIII] HSCT Hospital Surveillance
Common CMV, HSV, VZV Less common Adenovirus, influenza A, parainfluenza, RSV, Rhinovirus Rare Rotavirus, Coxsackie, polyoma virus Prophylaxis/Treatment Acyclovir Ganciclovir Foscarnet Avoidance Possible Treatments RSV Ig, ribavirin neuraminidase inhibitor, rimantadine Viral Infections after SCT
Community-Acquired Respiratory Virus Infections After Marrow Transplant:Fred Hutchinson Cancer Research Center (1990-1996) Respiratory syncytial virus 44 (35%) Parainfluenza 38 (30%) Type 1 18 Type 2 4 Type 3 16 Rhinovirus 31 (25%) Influenza 14 (11%) Type A 12 Type B 2 Bowden R. Am J Med 1997;102(3A):27-30.
9 8 7 6 5 Number of patients diagnosed 4 3 2 1 0 2 4 6 8 10 12 14 16 January February March April Week Respiratory Syncytial Virus Infection in Bone Marrow Transplant Patients Fred Hutchinson Cancer Research Center,1990 Harrington et al. J Infect Dis 1992;165:987-93.
1991 Community Influenza Outbreak Houston, TX • 27% of 15 HSCT outpatients and 29% of 28 HSCT inpatients with acute respiratory infections had documented influenza - mortality 17%. • 75% of all HSCT influenza cases during this outbreak were associated with pneumonia. • Risk factors for severe influenza disease include infection early after transplant just before engraftment of chronic GVHD. • Many acquired the infection while hospitalized Whimbey E. Bone Marrow Transplant 1994;13:437-40.
Viral Shedding for CRV Infections in HSCT Recipients Duration Infection up to 4 months influenza up to 2 years adenovirus up to 22 days RSV Note: RSV viral shedding has been reported to last 112 days in a child with SCID.
URI Recommendations HCWs and visitors with URI symptoms should be restricted from contact with HSCT recipients and candidates under-going conditioning therapy to minimize the risk for CRV transmission (AIII). Visitors with URI symptoms should be asked to defer their visit to the HSCT center until their URI symptoms resolve (BIII). All HCWs with URI symptoms should be restricted from patient contact and reassigned to non-patient care duties until their symptoms resolve (BIII).