Download
1 / 22
220 likes | 329 Views
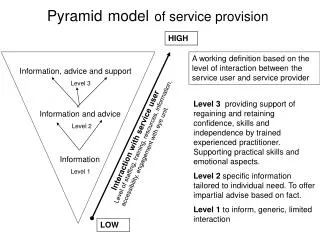
Findings and Recommendations. Operational Mapping of Health Service Provision in the Southern Zone of Tanzania. Management Team Meeting Richard Nkwera Dr. Oberlin Kisanga 15 th November 2011. Outline. Background and Objective Methodology Findings Issues and recommendations

E N D
Findings and Recommendations Operational Mapping of Health Service Provision in the Southern Zone of Tanzania Management Team Meeting Richard Nkwera Dr. Oberlin Kisanga 15th November 2011
Outline • Background and Objective • Methodology • Findings • Issues and recommendations • Way forward
Background and Objective • Gain insight of the Public and Private health services: in Lindi, Mtwara and Ruvuma • through assessment of location • service availability in view of rationalization potentials. • output and potential of health facilities • Transparency improvement among regional /zonal stakeholders for improved PPP • Service Rationalization: support informed Partnership decision making among: • location, • capacity and potential of health services (following key health problems), • physical infrastructure and catchment area • human resources and staff perspectives at governmental and private facilities
Methodology • 17 facilities physically visited others through regional/district respondents • Data assessment on district and hospital facility level • Quantitative • Questionnaires • Qualitative • Open ended questions • Focus group discussions • Desk review 5
Findings • Reference is made in respect to: • Lindi • Mtwara • Ruvuma • At the level of: • Regional • District /Council Hospital • Facility level
Health Facilities • Strong role and presence of faith based sector • MMAM requirement is almost three times of the available facilities (e.g. 181 to 496 Mtwara) • High number of health facilities - low number of skilled health workers • Over reliance of medical attendant – quality of services
Equipment and Infrastructure • Availability of beds • Rural hospitals have higher number of patients because of large catchment area and geographical location leaves patients with limited choice of hospital • The study recorded 2651 public and FBO inpatient hospital beds (public: 1,602; FBO: 1049) • In Lindi Region, for example, the faith-based sector operates 45% beds and Mtwara region in fact 63% of the beds are in faith-based hospital • Water and power supply: • Water – most facilities use piped • Electricity – mostly use of generator • General purpose Equipment – average - available and working • X-ray • Oxygen • Theater • Ambulance • Refrigerator etc. • Communications – limited internet access
Support Services • Laboratory Services • Basics (malaria) tests available • Advanced lab services – not available (sending samples for days) • Blood transfusing • Services available, though interruption reported to some districts in a period of three months (eg. Ruangwa and Liwale) • In all districts except for Tandahimba D.C relatives/friends or donors from the district are the main sources of blood donations, while Tandahimba the main type of donors are volunteers.
Patient disease specific interventions • Maternal and Child health interventions • Available at all facilities • Malaria services – available • Presumptive IPT for Malaria during pregnancy • HIV and AIDS, SRH and STI Services • Average: No SRH services targeting adolescents needs • Roman catholic facilities lack contraceptives • HIV counseling and testing – available • ART services – satisfactory (availability) • Overall SRH commodities - satisfactory
Human Resources • Density of medical doctors is very low • Ranging from 0.03 to 0.6 per 10,000 population • Backbone of services: midlevel cadres (AMO/CO - ENs) • Non professional: high number of Medical attendants • Specialists: nine (9) in the mapped area • Staff movement: from FBO to public
Human Resources Back bone of Health Services
Training • Per facility: • All health workers in each hospital received at least one training • At least one laboratory staff member trained in the diagnosis and treatment of malaria is less than 20% of facilities across the districts surveyed in Lindi and Mtwara Region. • At least one health worker in each hospital received the following trainings: • HIV and AIDS • Mother and Child Health • Reproductive Health • Malaria • Infection control • Tuberculosis Drug Management • Health Information Management System
Training Training Potentials: • High potential of the present institutions to cater for HRH development but No strategy for local demands. • shortage of tutors on top of the attrition due to retirement and disease burden is a challenge facing all the institutes e.g. in COTC Lindi, there are four tutors and two will be retired by year 2009/2010. • Recruitment of new tutors has not moved in proportion to student enrolment in most institutions. • Capacity to handle increased numbers of students and manage the condensed curriculum aimed at meeting MMAM targets is questionable as workload increase with no additional tutors
Partners Support • Presence - variety of stakeholders • Low coordination • Overlap esp. in HIV/A support • No support management plan • Mismatch between resource input with available Management capabilities. • Lindi • Clinton Foundation (CHAI) (HIVAIDS) • EGPAF – Care and Treatment • AGOTA • USAID • BIOSHAPE – HIV/AIDS Care and Treatment • BMAF – Staff support • Mtwara • JICA • BMAF • UNICEF • CHAI • EGPAF • Action Aid • Ruvuma • JICA • DANIDA • ITIAPOCUNICEF
Patients Movement (GIS) for normal delivery from wards to assessed health facility
Recommendations • Service provision • Where patients go to receive services? (avoid resource consuming duplication extensively explore the opportunities to invest in private service providers) • Recruit more national specialists to assure sustainability (as the majority of medical specialists identified in the study area were expatriates working on a short-contract basis) • Improve coordination of the few specialists available in the zone • Resources availability / facilities management • Human resources: • Retention measures should apply to both – public and private • Increase the availability of Assistant Medical Officers and maintain the relatively sound densities of enrolled nurses and clinical officers • The need for a more comparable system. (Districts use different staffing norms when calculating deficits for their Comprehensive Council Health Plans) • Health Training Institutions should have strategy to cater HRH local demands • Public and Private collaboration: • Enforcement of PPP
Way forward • Have TGPSH feedback • Linking stakeholders to these results • Building capacity of: • Regional referral • HRH • Government – informed decision making • What is available