Download
1 / 61
690 likes | 1.92k Views
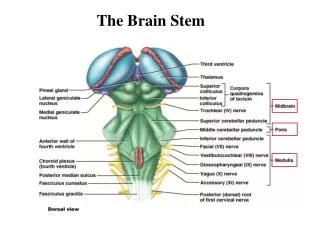
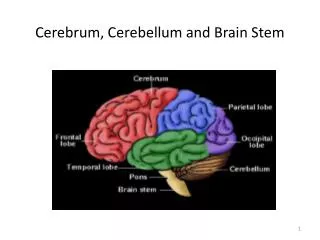
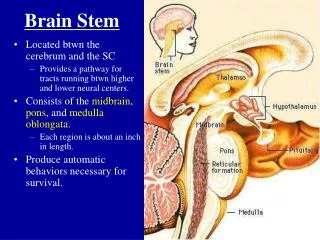
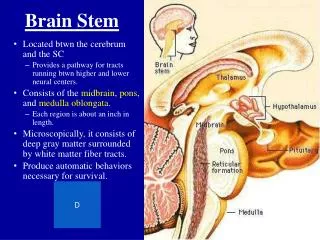
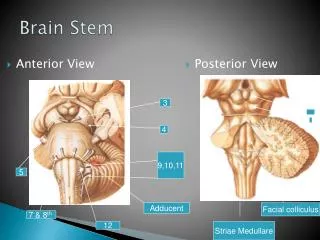
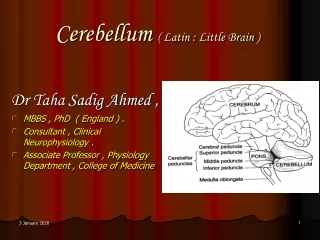
BRAIN STEM, CEREBELLUM and NEURO-OPTHALMOLOGY. Submitted to AskTheNeurologist.Com in 2007. GROSS ANATOMY . LATERAL VIEW. LOCATION OF CRANIAL NERVE NUCLEI WITHIN BRAINSTEM. CRANIAL NERVE 5.

E N D
BRAIN STEM, CEREBELLUM and NEURO-OPTHALMOLOGY Submitted to AskTheNeurologist.Com in 2007 AskTheNeurologist.Com
GROSS ANATOMY AskTheNeurologist.Com
LATERAL VIEW AskTheNeurologist.Com
LOCATION OF CRANIAL NERVE NUCLEI WITHIN BRAINSTEM AskTheNeurologist.Com
CRANIAL NERVE 5 Note that although all fibres enter the brainstem at the level of the pons, those concerned with pain and temperature descend as low as C3 AskTheNeurologist.Com
PATHWAYS INVOLVED IN HORIZONTAL GAZE LEFT FRONTAL EYE FIELD AskTheNeurologist.Com
INTERNUCLEAR OPTHALMOPLEGIA ( INO) AskTheNeurologist.Com
THE FACIAL NERVE Therefore a lesion at or distal to the facial nucleus will result in weakness of the upper as well as the lower part of the face:- this is what is know as a “ peripheral facial palsy ” AskTheNeurologist.Com
The Long Tracts Note sites of decussation of major tracts : Spinothalamic Cuneate / Gracile Corticospinal AskTheNeurologist.Com
LONG TRACT DECUSSATION • Spinothalamic Spinal cord • Gracile / Cuneate Medulla Medulla • Corticospinal Therefore: - Lesions at medulla and below can result in dissociated sensory syndromes - Lesions above the medulla will result in a contralateral upper motor neuron syndrome AskTheNeurologist.Com
The Corticobulbar Tract • Accompanies the corticospinal tract: can assume decussation occurs at level of nucleus • Connects with the brain-stem motor nuclei • Each tract connects bilaterally with most cranial nerve motor nuclei EXCEPT: Part of VII dealing with lower face is innervated unilaterally Sometimes XII innervated unilaterally AskTheNeurologist.Com
Lower motor neuron therefore signs of denervation present Tongue wasting and fasciculation Upper motor neuron therefore bilateral damage necessary Inappropriate spells of crying / laughing Jaw jerk and gag reflex increased Bulbar Palsy Pseudobulbar Palsy Dysarthria, dysphagia, weight loss, risk of aspiration pneumonia present in both cases AskTheNeurologist.Com
LATERAL MEDULLARY (WALLENBERG’S) SYNDROME LESION SITE IN LATERAL MEDULLARY SYNDROME ( BLUE) AskTheNeurologist.Com
VERTIGO, NYSTAGMUS VESTIBULAR NUCLEI CLINICAL FEATURES OF LMS I • IPSILATERAL HORNER’S SYNDROME • DESCENDING SYMPATHETIC TRACT • IPSILATERAL CEREBELLAR SIGNS • INFERIOR CEREBELLAR PEDUNCLE • DYSPHONIA AND DYSPHAGIA • NUCLEUS AMBIGUUS AskTheNeurologist.Com
CLINICAL FEATURES OF LMS II • LOSS OF IPSILATERAL FACIAL PAIN AND TEMPERATURE SENSATION • SPINAL TRACT AND NUCLEUS OF TRIGEMINAL NERVE • LOSS OF IPSILATERAL VIBRATION AND PROPRIOCEPTION IN LIMBS AND TRUNK • GRACILE AND CUNEATE NUCLEI AskTheNeurologist.Com
CLINICAL FEATURES OF LMS III • LOSS OF CONTRALATERAL PAIN AND TEMPERATURE SENSATION IN LIMBS AND TRUNK • SPINOTHALAMIC TRACT • HICCUPS • UNKNOWN • NUCLEUS AND TRACTUS SOLITARIUS • LOSS OF TASTE AskTheNeurologist.Com
Blood supply of Brainstem and Cerebellum • Ant. cerebral • Internal carotid • Middle cerebral • Post. communicating • Sup. cerebellar • Basilar • Ant. Inf. cerebellar • Vertebral • Ant. Spinal • Post. Spinal • Post. Inf. Cerebellar • Post cerebral • Mesencephalic AskTheNeurologist.Com
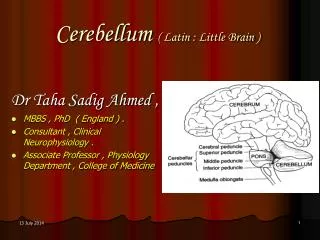
Somatotopy of cerebellum • Midline lesions: • nystagmus • Titubation • Trunk / gait ataxia • Hemispheric lesions: • nystagmus • ipsilateral limb signs posterior AskTheNeurologist.Com
Basic Plan of Cerebellar connections DN= Dentate nucleus T = Thalamus RN = Red nucleus Each cerebellar cortex controls ipsilateral side of body Efferents to cortex leave cerebellum via superior cerebellar peduncle Note: red nucleus is present in midbrain and ultimately controls contralateral half of body AskTheNeurologist.Com
DSCT= dorsal spinocerebellar tract VSCT= ventral spinocerebellar tract VSCT is crossed in the cord but crosses back within cerebellum AskTheNeurologist.Com
Fronto-ponto Cerebellar tract Right Cerebral cortex Note that right side of cortex ultimately controls left cerebellar hemisphere Fronto-ponto-cerebellar fibres enter cerebellum via middle cerebellar peduncle AskTheNeurologist.Com
Symptoms and signs of cerebellar disease (VANISH’D) • Vertigo • Ataxia - usually falls towards lesion • Nystagmus – increased with gaze towards lesion • Intention Tremor • Scanning speech • Hypotonia • Dysdiadochokinesia + Dysmetria AskTheNeurologist.Com
Approach to differential diagnosis of cerebellar dysfunction AskTheNeurologist.Com
Approach to localisation within brainstem A combination of long-tract and brainstem signs may allow accurate location of a brainstem lesion AskTheNeurologist.Com
Case 1* • Right facial paralysis affecting upper and lower face + diplopia + left hemiparesis ( arm and leg) • What is the likely cause of the diplopia and where is the lesion? AskTheNeurologist.Com
Answer 1 • Diplopia likely to be due to a right VIth nerve lesion – the VIIth nerve passes around the nucleus of VI just below the 4th ventricle in the pons • Right pons AskTheNeurologist.Com
Case2 • A 72 year old man with a right hemiplegia. On examination in addition to the hemiplegia with pyramidal signs his tongue deviates to the left and is atrophic and fasciculating on the left side AskTheNeurologist.Com
Answer 2 • Left medulla • Combination of XII LMN lesion on left, and right UMN hemiplegia places lesion in the left medulla above the decussation of the pyramidal tract AskTheNeurologist.Com
Case 3* • A 26 year old woman with horizontal diplopia on looking to left and right. On examination impaired adduction of both eyes on attempted lateral gaze with relative preservation of convergence. In addition dysmetria and intention tremor of right hand. AskTheNeurologist.Com
Answer 3 The patient has features of - a lesion of the medial longitudinal fasciculus bilaterally - a lesion of the right cerebellum ( or its connections) • A bilateral MLF lesion is almost pathognomonic of MS and the addition of cerebellar signs strengthens the diagnosis AskTheNeurologist.Com
Case 4 * • A 24 year old woman with vertical diplopia maximal on looking up and horizontal diplopia maximal on looking right, difficulty swallowing, ptosis more pronounced on left, facial weakness more pronounced on right. Sensation in tact. AskTheNeurologist.Com
Answer 4 • No single brainstem lesion can account for all these features. • Myaesthenia gravis may present in this way with a combination of pure motor signs attributable to NMJ dysfunction of muscles innervated by various brainstem nuclei. AskTheNeurologist.Com
Case 5* • A 65 year old lady with a right sided ptosis, right pupil dilatation, diplopia, left sided cerebellar and pyramidal signs AskTheNeurologist.Com
Answer 5 • Right Midbrain • Eye signs are due to right III palsy. • Contralateral cerebellar signs due to damage to right Red Nucleus • Contralateral pyramidal signs due to damage to corticospinal tract AskTheNeurologist.Com
Case 6* • A 84 year old lady with sudden onset of a left hemiparesis and deviation of both eyes to the left side AskTheNeurologist.Com
Answer 6 • Right pons • The combination of gaze deviation and hemiparesis usually occurs with large hemispheric CVA’s; in such a case the eyes deviate to the side of the lesion ( due to destruction of the frontal gaze centre) • In case 8 the eyes deviate away from the lesion (left) due to the destruction of the right pontine paramedian reticular formation (PPRF) AskTheNeurologist.Com
What is Nystagmus? • Rhythmic oscillation of the eyes • Fast phase ( saccade) • Slow phase ( smooth-pursuit – like) AskTheNeurologist.Com
Describing nystagmus • Position of gaze in which occurs or is most prominent • Direction ( of FAST phase) • Precipitating / exacerbating factors • Fatiguing / persistent • Associated symptoms - Vertigo - Oscillopsia – feeling that vision is jerky AskTheNeurologist.Com
Example: - Vestibular neuronitis left side • Most prominent on gaze towards right • Horizontal right – sided nystagmus with a rotatory component • Exacerbated by quick head movements • Associated with severe vertigo + / - vomiting • Persistent / may fatigue Illustrates following rule: Nystagmus is always most prominent on gaze towards the direction of the fast phase AskTheNeurologist.Com
Nystagmus may be……… • Physiological • Pathological Central Peripheral this is THE most important distinction to be made in assessing nystagmus! AskTheNeurologist.Com
IS IT NORMAL?? AskTheNeurologist.Com
Central vs Peripheral ( guidelines) AskTheNeurologist.Com
Diplopia “ The subjective feeling of seeing double” May be: • Monocular ( present even when one eye open) • Binocular ( present only when 2 eyes open) Monocular diplopia is either due to a local (ocular) process, “non-organic” in origin or very rarely from visual cortical dysfunction Therefore almost all neurological causes of diplopia are “ binocular ” AskTheNeurologist.Com
Binocular diplopia…questions • Horizontal vs Vertical ? • Worse on looking in which direction? • Worse on focussing near or far ? • RULES • Diplopia is maximal on gaze in the direction of action of the weak muscle. • The false image is projected towards the direction of action of the weak muscle AskTheNeurologist.Com
Anatomical sites which may cause diplopia • Internuclear ( INO ) • Nucleus • Fascicle • Cranial nerve • Neuromuscular junction (NMJ)*** • Muscle • Local distortion of orbit *** ANY type of diplopia or gaze disturbance may be due to a problem at the NMJ….usually Myaesthenia Gravis …and often with ptosis AskTheNeurologist.Com
Example of a patient with Myaesthenia Gravis The examiner is lifting the patient’s eyelids for 2 reasons: - Good examination technique! - In this case the patient has bilateral ptosis AskTheNeurologist.Com
Which of the following patients cannot have MG? • Right eye totally paralysed, left eye moves freely but with ptosis • Inability of both eyes to move to left with no diplopia • Bilateral inability to look up with bilateral ptosis • Left eye deviated down and laterally with ptosis on left and left pupil larger than right Myaesthenia Gravis NEVER causes pupil asymmetry ( anisocoria) …..which brings us onto the next subject….. AskTheNeurologist.Com
Anisocoria “ Inequality between the 2 pupils” Pupils may be : - equal ( to within 1mm) - unequal due to surgery / trauma usually irregular) - unequal due to a neurological condition AskTheNeurologist.Com
The 2 neurological causes of anisocoria • One pupil too big • One pupil too small Parasympathetic---------------------------------------Sympathetic Constricts (Ach) Travels in III Dilates (Nad) Symp fibres AskTheNeurologist.Com
Anisocoria rules • Darkness exaggerates failure of dilation • Bright light exaggerates failure of constriction • If unilateral ptosis is present assume that the eye with the ptosis is sick! AskTheNeurologist.Com