Download
1 / 46
511 likes | 1.31k Views
Current Management of Children with Appendicitis. George W. Holcomb, III, M.D., MBA Surgeon-in-Chief Children’s Mercy Hospital Kansas City, Missouri. Surgical History for Appendicitis. Reginald Fitz: pathologist 1886 – Described pathology of the appendix Termed the disease: appendicitis

E N D
Current Management of Children with Appendicitis George W. Holcomb, III, M.D., MBA Surgeon-in-Chief Children’s Mercy Hospital Kansas City, Missouri
Surgical History for Appendicitis • Reginald Fitz: pathologist • 1886 – Described pathology of the appendix • Termed the disease: appendicitis • Charles McBurney: surgeon • 1889 – Described classical sign for appendicitis • Kurt Semm: gynecologist and engineer • 1981 – 1st laparoscopic appendectomy
Surgical History for Appendicitis 1990 – 2000 • Slow adoption for laparoscopic approach • Why – • Relatively small open incision (c/w splenectomy, fundoplication, cholecystectomy) • Many cases done middle of night – OR crews not used to laparoscopy • Benefits were not well appreciated
Surgical History for Appendicitis 2000 – 2010 • Laparoscopic approach now favored (exclusively used at many centers including CMH) for all conditions: acute, perforated, abscess • Why • Operative times improved – closure faster • Significantly fewer wound infections (almost none) • Improved cosmesis, esp if infection develops
Laparoscopic AppendectomyTechnique • Window in mesoappendix • Vascular stapler across mesoappendix
Acute Appendicitis(No Perforation) • April 2003 – Nov 2006 • 609 Pts – laparoscopic appendectomy • 3 post-op abscesses (0.49%)
Acute Appendicitis Appendiceal Perforation • Perforated appendicitis (3 - 5 day hx) • Evacuation/irrigation of purulent material • Wound problems minimized • 20% post-op abscess rate
Laparoscopic Appendectomy Please use this link if you experience problems viewing the video above.
Laparoscopic vs Open AppendectomyPerforated Appendicitis • Far fewer (almost none) wound infection with laparoscopic approach • Allows surgeon to suction/irrigate under direct visualization • Less postoperative SBO
Adhesive Small Bowel Obstruction After Appendectomy in Children: Comparison Between the Laparoscopic and Open Approach AAP 2006 J PediatrSurg 42:939-942, 2007
Laparoscopic versus Open Appendectomy(1105 Patients) AAP 2006 J PediatrSurg 42:939-942, 2007
SBO After Perforated Appendicitis(378 Patients) AAP 2006 J PediatrSurg 42:939-942, 2007
2000 – 2012 Questions • Do we operate in the middle of the night? • Is there an optimal antibiotic regimen for perforated appendicitis? • How do we define perforated appendicitis? • How do we manage the patient presenting with an abscess? • Which is better: SSULS or 3 port appendectomy?
When to Operate?Current Practice at CMH • Patients identified with appendicitis are booked for laparoscopic appendectomy • All receive a dose of rocephin (50mg/kg) and flagyl (30mg/kg) • This antibiotic regimen was shown to be most cost effective in PRT • If patients present at night, the operations are scheduled for the ‘surgeon of the week’ the next day (8 am or 1 pm start) • Appendectomies rarely occur after 10 PM at night
Operation at Presentation Versus The Following Day Yardeni D, Hirschl RB, Drongowski RA, et al: Delayed versus immediate surgery in acute appendicitis: Do we need to operate during the night? J PediatrSurg 39:464-469, 2004. • Retrospective comparison in children (Level 3 study) between operation < 6 hrs after presentation or the following day • 126 patients (38 early vs 88 late) • No differences in operating time, perforation rate, or complications
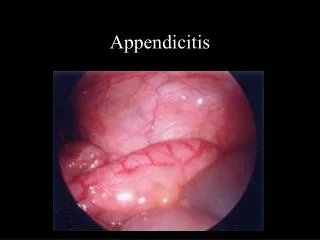
Definition of Perforation Used in Prospective Randomized Trial Visible appendicolith Hole in appendix
Post-operative Antibiotic Regimen For Perforated Appendicitis In Children: A Prospective Randomized Trial • April 2005 - November 2006 • 100 patients • To ensure accurate data, the two groups had to be equal and a definition had to be created
Hypothesis • A correct definition of perforation (DOP) is important because • Provides us with the information to safely and efficiently treat patients • Allows us to better identify which patients are at risk for developing postoperative complications • If our definition of perforation was correct • There should be no increase in abscess rate in the cohort of patients treated as non-perforated appendicitis after the definition was used • If our definition of perforation was incorrect • There should be an increase in abscess rate in the cohort of patients treated as non-perforated appendicitis after the definition was used (b/c of under-treatment)
ResultsOutcomes PAPS 2008 J PediatrSurg 43:2242-2245, 2008
Conclusions • Our strict DOP (either a visible hole in the appendix or appendicolith in the abdomen) has been shown to be safe • No increase in abscess rate for non-perforated patients • No detectable risk of under treating patients defined as non-perforated • This DOP will improve overall care for children with appendicitis • Eliminate unnecessary antibiotic treatment • Improve cost management • Simplify treatment protocols • Improve the integrity of clinical data • Allow for ongoing clinical research PAPS 2008 J PediatrSurg 43:2242-2245, 2008
How do we manage the child presenting with an abscess due to ruptured appendicitis?
Perforated AppendicitisPresenting With Abscess History • Open operation for abscess is difficult • Percutaneous drainage has been described and applied • Laparoscopy is being used to treat perforated appendicitis and abscess • Which is better?
Acute Appendicitis • 5 - 7 day history • Dehydrated – needs IVF • Percutaneous drainage (interventional radiology) • PICC line - antibiotics • Discharge day 3-5 if stable • Antibiotics con’t 10 - 14 days at home • Return 8-10 wk. for interval appendectomy (to prevent recurrent appendicitis) - overnight hospitalization
Retrospective Experience with Interval Appendectomy • 52 patients – 2000-2006 • Total hospital days = 7.0 +/- 3.9 • Total healthcare visits = 7.6 +/- 2.8 • Total number of CT scans = 3.5 +/- 2.0 • Recurrent Abscess = 10 pts (19.2%) AAP, 2007 JPediatrSurg 43:981-985, 2008
Abscess StudyProspective Trial • Drainable abscess • OR for laparoscopic appendectomy vs percutaneous drainage as initial management • Drain groups undergoes laparoscopic appendectomy at 10 weeks. • Quality of life surveys at admission, at 2 weeks and at 12 weeks • Pilot study – 40 patients APSA 2009 J PediatrSurg 45:236-240, 2010
Initial Non-Op Mgmt vs Lap Appendectomy in Children Presenting with an Abscess Values are expressed as mean ± SD APSA 2009 J PediatrSurg 45:236-240, 2010
Initial Non-Op Mgmt vs Lap Appendectomy in Children Presenting with an Abscess Values are expressed as mean ± SD, unless otherwise indicated APSA 2009 J PediatrSurg 45:236-240, 2010
Prospective Randomized Trial • Conclusion – There is no difference b/w initial laparoscopic operation vs initial non-operative management followed by laparoscopic interval appendectomy • Management can be determined by the surgeon’s preference and experience APSA 2009 J PediatrSurg 45:236-240, 2010
Is there an advantage performing the laparoscopic appendectomy through a single umbilical incision?
SSULS Appendectomy Please use this link if you experience problems viewing the video above.
Prospective Randomized Trial Single Umbilical Incision vs 3-PortLaparoscopic Appendectomy • 360 total patients • Acute non-perforated appendicitis • August 09 – November 10 • Primary outcome variable – postoperative wound infection • Standardized pre and postoperative management • Quality of life surveys at 6 weeks and 6 months ASA, 2011 Ann Surg 254:586-590, 2012
Patient Characteristics at Operation ASA, 2011 Ann Surg 254:586-590, 2012
Outcome Data ASA, 2011 Ann Surg 254:586-590, 2012
Other Outcomes ASA, 2011 Ann Surg 254:586-590, 2012
Convalescence Following Discharge ASA, 2011 Ann Surg 254:586-590, 2012
Subset Analysis • BMI% for age & gender: overweight 85-95%, obese >95% • Compared normal to overweight and normal to obese within each group • Compared single site to 3 port within each body habitus classification IPEG 2012
Technique Comparison For Overweight IPEG 2012
Technique Comparison For Obese IPEG 2012
Conclusions • Obesity increases operating time, postoperative length of stay, doses of narcotics, and hospital charges with single site lap appendectomy • Obesity has no impact in 3 port appendectomy • Clinically significant increase in wound infection in overweight and obese patient undergoing single site lap appendectomy • We do not recommend single site laparoscopic appendectomy in obese patients IPEG 2012
Summary • There have been significant changes in the surgical management of appendicitis • These changes have revolved around timing of surgery and the almost exclusive use of the laparoscopic approach • Unclear if appendicitis will be a surgical disease in the future
QUESTIONS www.cmhclinicaltrials.com www.cmhmis.com