Download
1 / 116
1.18k likes | 1.38k Views
ASSESSMENT AND MANAGEMENT OF IgA NEPHROPATHY John Feehally. IgA NEPHROPATHY The commonest pattern of glomerulonephritis in the world. CLASSIFICATION OF GLOMERULONEPHRITIS. Histopathology. Clinical. Immune mechanisms. CLASSIFICATION OF GLOMERULONEPHRITIS. Histopathology. Clinical.

E N D
IgA NEPHROPATHYThe commonest pattern of glomerulonephritis in the world
CLASSIFICATION OF GLOMERULONEPHRITIS Histopathology Clinical Immune mechanisms
CLASSIFICATION OF GLOMERULONEPHRITIS Histopathology Clinical Immune mechanisms Patterns established on light microscopy Membranous Membranoproliferative Focal segmental glomerulosclerosis etc……
CLASSIFICATION OF GLOMERULONEPHRITIS Histopathology Clinical Immune mechanisms Patterns established on light microscopy Membranous Membranoproliferative Focal segmental glomerulosclerosis etc…… ‘Patterns’ not ‘diseases’
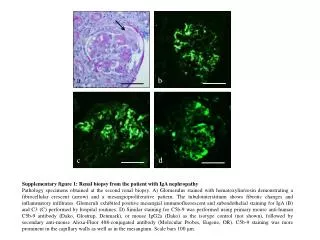
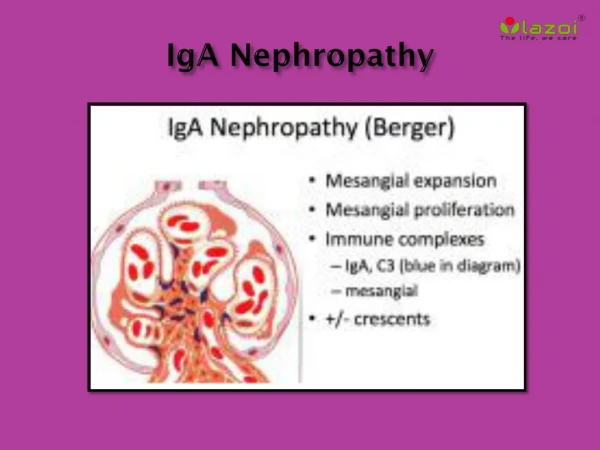
IgA1 deposition In the glomerular mesangium
ASSESSMENT AND MANAGEMENT OFIgA NEPHROPATHYIs IgA nephropathya single ‘disease’ ?
IgA NEPHROPATHYA pattern of glomerulonephritis with many variations
Recurrent visible haematuria Coincides with mucosal infection
Asymptomatic Haematuria / proteinuria
CKD Proteinuria Hypertension Renal impairment
‘SECONDARY’ IgA NEPHROPATHY COMMONLY REPORTED ASSOCIATIONS Alcoholic liver disease Celiac disease Ankylosing spondylitis Reiter’s syndrome Uveitis Dermatitis herpetiformis
RECURRENT IgA NEPHROPATHY Pooled published data – 5 year follow up Recurrence 38-60% Graft dysfunction due to recurrence 15% Graft loss due to recurrence 7%
RECURRENT IgA NEPHROPATHY Pooled published data – 5 year follow up Recurrence 38-60% Graft dysfunction due to recurrence 15% Graft loss due to recurrence 7% Why does IgA nephropathy NOT always recur ?
15-21% 4.7% <5% Percentage of patients with primary glomerular disease
15-21% Male > Female Male = Female 4.7% <5%
IgA NEPHROPATHYVariations in: Pathological pattern Clinical pattern Transplant recurrence Epidemiological patternPathogenesis
IgA NEPHROPATHY Not expect a single pathogenic mechanism to lead to mesangial IgA deposition and injury No proof that IgAN is a single ‘disease’ No proof that IgAN is the same ‘disease’ in all parts of the world
ASSESSMENT AND MANAGEMENT OFIgA NEPHROPATHY Can you predict which patients with IgA nephropathywill get kidney failure?
ASSESSMENT AND MANAGEMENT OFIgA NEPHROPATHYCan you predict which patients with IgA nephropathywill get kidney failure?CLINICAL evidence
PROGNOSIS IN IgA NEPHROPATHY Rodicio 1982
PROGNOSIS IN IgA NEPHROPATHY 20% ESRD @ 20 years Rodicio 1982
IgA NEPHROPATHY IN INDIA CMC Vellore 1994-2003 Chacko B et al. Nephrology 2005; 10: 496
IgA NEPHROPATHY IN INDIA CMC Vellore 1994-2003 478 adults 55% - Nephrotic syndrome at presentation 56% - Serum creatinine > 123 μmol/L at presentation Chacko B et al. Nephrology 2005; 10: 496
MACROSCOPIC HAEMATURIA AND PROGNOSIS IN IgA NEPHROPATHY Beukhof 1983
LEAD TIME BIAS IN DIAGNOSIS OF IgA NEPHROPATHY Geddes CC et al. NDT 2003; 18: 1541
ISOLATED NON-VISIBLE HAEMATURIA IN IgA NEPHROPATHY How benign is it ? Cohort study – Toronto – 286 patients Proteinuria < 0.2 g/24hr Normal BP Non-visible haematuria plus Bartosik et al. AJKD 2001; 38: 728
ISOLATED MICROSCOPIC HAEMATURIA IN IgA NEPHROPATHY How benign is it ? Cohort study – Toronto – 286 patients Proteinuria < 0.2 g/24hr Normal BP Microscopic haematuria plus 10 year risk of deterioration in renal function = ZERO Bartosik et al. AJKD 2001; 38: 728
ISOLATED NON-VISIBLE HAEMATURIA IN IgA NEPHROPATHY How benign is it ? Cohort study – Hong Kong Non-visible haematuria Proteinuria < 0.4 g/24hr plus During 7 years follow up, 44% had a ‘clinical event’ 33% proteinuria 26% hypertension 7% renal impairment Szeto C et al Am J Med 2001; 110:434
OUTCOME AND AVERAGE FOLLOW-UP PROTEINURIA IN IgA NEPHROPATHY
REMISSION OF PROTEINURIA IMPROVES PROGNOSIS IN IgA NEPHROPATHY • Time-average proteinuria • 1 - < 1g/24h • 2 – 1-2 g/24h • 3 – 2-3g/24h • 4 - >3g/24h Reich H et al. JASN 2007; 18: 3177
ASSESSMENT AND MANAGEMENT OFIgA NEPHROPATHYCan you predict which patients with IgA nephropathywill get kidney failure?PATHOLOGICAL evidence
A CLINICO-PATHOLOGICAL CLASSIFICATION FOR IgA NEPHROPATHY • Does pathology add prognostic information • .. to clinical data at time of biopsy ? • .. to clinical data during follow up ?
A CLINICO-PATHOLOGICAL CLASSIFICATION FOR IgA NEPHROPATHY • Does pathology add prognostic information • .. to clinical data at time of biopsy ? • .. to clinical data during follow up ? Perhaps the biopsy is only useful to establish the diagnosis of IgAN ?
PATHOLOGICAL CLASSIFICATIONS IN RENAL DISEASE Are usually based on expert opinion ... and pre-conceived ideas of what lesions are important
OXFORD CLASSIFICATION OF IgA NEPHROPATHY A different way Approach the problem with an open mind With an international consensus group • Study all histological lesions • Test reproducibility & independence • Then test correlations with outcome
SCORING OF SELECTED PATHOLOGY FEATURES Mesangial hypercellularity - in > or <50% of glomeruli M0 or M1 Endocapillary hypercellularity – present/absent E0 or E1 Segmental sclerosis/adhesions – present/absent S0 or S1 Tubular atrophy/interstitial fibrosis – 0-25%, 26-50%, >50% T0 or T1 or T2 Each can be scored easily in routine clinical practice
PREDICTIVE SIGNIFICANCE OF PATHOLOGY FEATURES IN IgA NEPHROPATHY • M E S T • Each adds predictive value to …. • Initial clinical features • Follow up clinical features In all ages and races studied
VALIDATION STUDIES FOR THE OXFORD CLASSIFICATION OF IgAN
WHAT NEXT ? Validation studies Work towards combining pathology and clinical elements – to produce a single ‘risk score’ There is now the opportunity to design smaller, shorter RCTs
ASSESSMENT AND MANAGEMENT OFIgA NEPHROPATHYHow good is the evidence to guide the treatment of IgA nephropathy ?
KI Supplements 2012 2(2): 1-274 CLINICAL PRACTICE GUIDELINE FOR GLOMERULONEPHRITIS
Examples of Rating Guideline Recommendations QUALITY of Supporting Evidence is shown as A, B, C or D