Download
1 / 42
430 likes | 562 Views
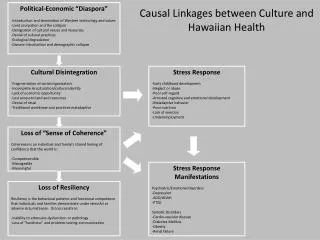
Modelling the Linkages Between Cannabis and Psychotic Symptoms. Christchurch Health & Development Study Christchurch School of Medicine & Health Sciences. D Fergusson L J Horwood E M Ridder J M Boden. INTRODUCTION.

E N D
Modelling the Linkages Between Cannabis and Psychotic Symptoms Christchurch Health & Development Study Christchurch School of Medicine& Health Sciences D Fergusson L J HorwoodE M Ridder J M Boden
INTRODUCTION Psychosis refers to severe mental illness characterised by the presence of delusions, hallucinations and other associated cognitive and behavioural impairments that grossly interfere with the ability to meet the ordinary demands. The most well known psychosis is schizophrenia
INTRODUCTION (Cont) Interest in the linkages between cannabis use and the development of psychosis or psychotic symptoms can be traced back to the Indian Hemp Commission of 1894. However, modern interest in this topic can be traced to a study conducted in 1987 by Andreasson and colleagues who looked at the relationship between cannabis use at 18 and later psychosis in a large sample of Swedish conscripts. This study found elevated rates of psychosis amongst those reporting cannabis use.
OTHER RESEARCH Since Andreasson’s original study there have been a series of prospective studies that have examined the link between the use of cannabis and the development of psychosis or psychotic symptoms. These studies include: Arseneault et al, 2002; Fergusson et al 2003; Van os et al, 2002; Henguet et al 2005; Caspi et al 2005; Zammit et al 2002; Stefanis et al 2004. In all studies, the use of cannabis has been found to be associated with increased rates of psychosis or psychotic symptoms.
KEY ISSUES Whilst longitudinal studies have clearly established a correlation between the use of cannabis and later psychosis, there have been ongoing debates about the extent to which this association reflects a causal relationship. Two major threats to validity have been raised. 1. Confounding. It has been proposed that the association arises because of third or confounding factors that are correlated with cannabis use and are also related to the development of psychosis. While existing research has controlled a large number of potential confounders, it may be proposed that the association reflects non observed uncontrolled confounding (McCleod et al 2004).
KEY ISSUES (Cont) 2. Reverse Causality: A second explanation is that the association may arise from self medication in which those with psychosis are more prone to use cannabis than other individuals.
AIMS In this presentation I will describe the findings of a study in which we aimed to control non observed confounders and reverse causality.
CHRISTCHURCH HEALTH AND DEVELOPMENT STUDYAN OVERVIEW • Initial Study Group (cohort): All children born in the Christchurch urban region during April to August 1977. • Number studied: 1,265. • Ages studied: Birth, 4 months, 1 year, annual intervals to 16 and again at ages 18, 21 and 25.
CHRISTCHURCH HEALTH AND DEVELOPMENT STUDYAN OVERVIEW (Cont) • Source of Information: Parents, School Teachers, Children, Official Records. • In general terms, the study has aimed to provide a running record of the social background, health and development of a large group of Christchurch born children as they move from infancy into adulthood.
SAMPLE RETENTION At age 25, a total of 1,003 participants was studied. This sample represented 79% of the original cohort and 90% of the cohort resident in New Zealand.
MAIN MEASURES 1. Self reported use of cannabis at: 17-18, 20-21 and 24-25 years. 2. Rates of psychotic symptoms assessed using the SCL90 at 18, 21, 25 years.
ASSOCIATIONS BETWEEN CANNABIS USE AND PSYCHOTIC SYMPTOMS(18, 21, 25)
COVARIATE ADJUSTMENT MODELS Model 1: Population averaged model. Log (Yit) = B0 + B1 Xit + Bj Zij + Bk Wikt + Eit Where Yit is the rate of symptoms for the ith participant, Xit is cannabis use at time t, Zij were a set of fixed covariates and Wkit a set of time dynamic factors. This model was estimated using GEE estimation that assumed that the covariance matrix of the disturbances Eit was unconstrained.
COVARIATE ADJUSTMENT MODELS Model 2: Random effects. Log (Yit) = B0i + B1 Xit + Bj Zij + Bk Wikt + Eit Where B0i was an individual specific intercept that was assumed to be uncorrelated with Xit, Zij and Wikt.
COVARIATE ADJUSTMENT MODELS Model 3: Fixed effects. Log (Yit) = B0i + B1 Xit + Bk Wikt + Eit Where B0i is an individual specific intercept which represents fixed factors influencing Yit. B0i is permitted to be correlated with Xit and Wikt.
THE FIXED EFFECTS MODEL An important feature of the fixed effects model is that it controls all non observed fixed factors that may confound the relationship between Yit and Xit. To understand how the model achieves this, it is easiest to work with an illustrative OLS model.
ILLUSTRATIVE MODEL Consider the same cohort observed on measures of cannabis (Xt) and symptoms (Yt) on two occasions. To describe the linkages between Xt and Yt we propose the model. Y1 = B0 + B1 X1 + U + E1 Time 1 Y2 = B0 + B2 X2 + U + E2 Time 2 Where U represents non observed fixed confounding factors that may be correlated with Xt.
ESTIMATION It proves straightforward to estimate B1 in a way that does not depend on the knowledge of U. Y1 = B0 + B1 X1 + U + E1 Y2 = B0 + B1 X2 + U + E2 (Y1 - Y2) = B1 (X1 - X2) + (E1 - E2)
THE FULL FIXED EFFECTS MODEL The principles above generalise to multiple time points: (Yit - y) = B1 (Xit - x) + (Eit - e) When y, x, e are the subject specific means of Yit, Xit and Eit respectively.
THE FULL FIXED EFFECTS MODEL (Cont) While the fixed effects model controls for fixed sources of confounding it does not control for time dynamic factors. The model can be extended to include observed time dynamic factors. (Yit - y) = B1 (Xit - x) + Bk (Wikt - w) + (Eit - ei) Methods for estimating coefficients using logit, poisson and negative binomial models have been developed.
ASSOCIATIONS BETWEEN CANNABIS USE AND PSYCHOTIC SYMPTOMS ADJUSTED FOR COVARIATES
ASSOCIATIONS BETWEEN CANNABIS USE AND PSYCHOTIC SYMPTOMS ADJUSTED FOR COVARIATES (Cont) All models show that after adjustment for confounders daily users of cannabis had rates of symptoms that were between 1.6-1.8 times higher than non users.
RECIPROCAL CAUSAL MODEL Although the covariate adjustment models show that cannabis use and symptoms are related to each other net of common confounders, these analyses do not establish the direction of causation. Here there are two possibilities. Symptoms Cannabis In the next stage of the analysis we used structural equation modelling methods to explore the direction of causation.
ADDRESSING REVERSE CAUSALITY To examine reverse causality we extended the analysis to fit the multivariate model.
MODEL EQUATIONS Although the model path diagram is complex the underlying algebraic structure is straightforward. The kernel of the model (leaving aside disturbance assumptions) involved two sets of equations. The first set of equations explain the fixed sources of variation influencing: a) symptoms Pt; and b) cannabis use Ct. These equations are: Ct = C + Ut Pt = P + Wt Where P and C are latent fixed effects factors. The model permits P and C to be correlated.
MODEL EQUATIONS (Cont) The second set of equations model the relationship between symptoms and cannabis net of the fixed effects P, C. Ut = B1 Wt + Btu Ut-1 + t Wt = B2 Ut + Btw Wt-1 + t We permit the disturbances t, t to be correlated within time period t.
IDENTIFICATION For 3 time periods, with measures of cannabis Ct and symptoms Pt observed at each time, this model is identified and has 5 df. The model was estimated in LISREL using weighted least squares methods to take account of the non normality of data.
MODEL INTERPRETATION While the model structure is complex, there are only two parameters of interest: 1. B1 which describes the effects of psychosis on cannabis use. 2. B2 which describes the effects of cannabis use on psychosis.
RECIPROCAL CAUSES MODEL The results of the structural equation model (below) showed: i) The use of cannabis was associated with significant increases in rates of psychotic symptoms. ii) Psychotic symptoms did not lead to an increase in cannabis use.
EVIDENCE IN FAVOUR OF A CAUSAL LINK 1. Association: All studies of general population samples have found increased rates of psychosis/ psychotic symptoms amongst cannabis users. 2. Dose/Responses: Increasing use is associated with increasing risk.
EVIDENCE IN FAVOUR OF A CAUSAL LINK (Cont) 3. Resilience to Confounding: In all studies associations between cannabis and psychosis/ psychotic symptoms have persisted following control for confounding. 4. Control for Reverse Causality: All studies to date have found that the association cannot be explained by reverse causation in which psychosis leads to the use of cannabis.
EVIDENCE IN FAVOUR OF A CAUSAL LINK (Cont) 5. Measurement: Associations have been found using both diagnoses of psychosis and scale score measures of psychotic symptoms.
SIZE OF EFFECT While all studies suggest a possible causal link between cannabis and psychosis, the size of the association is relatively small. Estimates suggest that elimination of all cannabis use could reduce overall rates of psychosis by 10%. One reason for the small effect size may be that only minority of the population are susceptible to the effects of cannabis.
IMPLICATIONS FOR PROHIBITION/LEGALISATION OF CANNABIS Findings on the link between cannabis and psychosis have been used to argue against attempts to liberalise cannabis laws. As with all issues in the cannabis debate, matters are not straightforward.
ARGUMENT AGAINST LIBERALISATION It could be suggested that since the use of cannabis may lead to psychosis in susceptible individuals, there are grounds for opposing the liberalisation of the cannabis laws.
ARGUMENT FOR LIBERALISATION It could also be suggested that since the effects of cannabis on psychosis are small, this link does not provide grounds for opposing liberalisation. The majority of recreational cannabis users do not appear to suffer harmful effects and at current levels of use, cannabis is less harmful than alcohol or tobacco.
WEIGHING THE EVIDENCE As in all aspects of the cannabis debate, the arguments for and against cannabis legalisation involve weighing the rights of the majority for whom cannabis use is not harmful against the risk of the minority who experience adverse consequences.
CONCLUDING COMMENTS While the analysis I have described above has been applied to the issue of cannabis and psychosis, these techniques may be readily adopted to criminological analyses. Examples that come to mind include: peer affiliations and crime; alcohol and crime, etc.
CAVEATS However, as with all techniques, knowledge is purchased at the cost of underlying assumptions that may or may not be realistic. The methods I describe have the following points of vulnerability. i) In the fixed effects model, it is critical that change in both the outcome and exposure variable is non trivial. Because the model relies on differences in variables, standard errors are increased and statistical precision is reduced.
CAVEATS (Cont) ii) The SEM approach relies on the assumption that all of the available evidence is adequately summarised in the variance/covariance matrix. This may not always be a realistic assumption. Furthermore, there are unresolved concerns and issues about fitting linear models to highly skewed non normal data.
FINAL COMMENT Whilst there is a need for some skepticism about the extent to which fixed effects and SEM can address issues relating to non observed confounders and causal directions, these methods appear to be the best available at the present time. They at least may provide preliminary answers to these complex issues.