Download
1 / 12
150 likes | 504 Views
APERT SYNDROME. BY Milana Abayev DEN2311/D246 11/26/15. Apert syndrom. It is a rare type I genetic disorder characterized by premature fusion of skull ( craniosynostosis). It affects the normal growth of head and face and also extremities such as fused figures and toes (syndactyly).

E N D
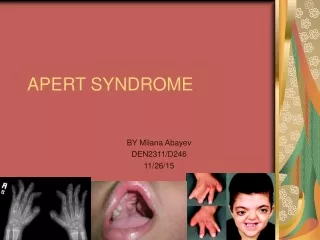
APERT SYNDROME BY Milana Abayev DEN2311/D246 11/26/15
Apert syndrom • It is a rare type I genetic disorder characterized by premature fusion of skull ( craniosynostosis). • It affects the normal growth of head and face and also extremities such as fused figures and toes (syndactyly). • Its happens due to the mutation of a gene called FGFR2, which produces a protein called fibroblast growth factor receptor 2. This gene stimulates constant signals that causes premature cells to become bone during embryonic phase.
Epidemiology: • It’s an autosomal dominant trait ( which means that only one parent is needed to pass on the defective gene). • It can happen sporadically to parents with no history of the disorder or with affected individuals which have 50% chance to pass it to their offspring's. • Male above the age 50 have a higher risk of having the defective gene. • It found in 1 in 65,000 to 88,000 newborns
Facial characteristics of Apert syndrome: • Sunken appearance of middle of the face. • Bulging and wide set of eyes • Depressed nasal bridge with beaked nose appearance. • Undeveloped upper jaw
Other Charecteristics of Apert Syndrome: • Fusion of fingers and toes • Short height • Hearing loss and frequent ear infections • Intelligence varies from normal to mental deficiency • Hyperhidrosis • Paronychial infections • Cardiovascular defects • Polycystic kidneys • Preventable visual loss • Optic atrophy • Sleep apnea • Patient might have social problems • Self-esteem problems
Trapezoid shaped mouth at rest Maxillary hyperplasia Lateral palatal swellings Gingival hypertrophy Multiple tooth agenesis Shovel shaped incisors High carries prevalence Early tooth loss Poor oral hygiene Maxillary crowding Malocclusion Delayed dentition V shaped maxillary arch Bifid uvula Cleft palate Bulging alveolar ridge Dentitio tarda Some impacted, partial eruption teeth Idiopthaic root resorption Supernumerary teeth Transposition of tooth germs Oral manifestations:
Prognosis: • Children require usually surgery to separate skull bones to allow for the brain to develop normally as possible • The surgery is usually done at early stages; the older the child, the the less chances he has to develop normal intellectual ability • Even with a early surgery, certain brain structure do not develop normally. • Usually children who are raised by their parents have a higher chance of achieving normal intellectual capability. • 4 out of 10 kids have normal IQ. • About 18 institutionalized children reach normal IQ • 3 out of 136 children will be able to attend college • Life expectancy varies between children
Treatment: • Since most the syndrome is sporadic, genetic testing is ineffective • If the carrier of the gene (affected individual) would like to reproduce offspring then genetic testing is recommended • No treatment is known to avoid the syndrome or treat it • Surgery is not a treatment of the disease, its only use is to better the quality of life of the individual • The first surgery would be to correct the abnormal bone growth of the skull at early stages of life (6-8 months). This procedure is necessary to relive pressure on the brain and provide brain growth, normal as possible • As the child grows facial bones again they become misaligned, a surgeon will perform another surgery to align the bones in to normal position (usually at age 4-12) • Corrective surgery might be required to fix the fussed fingers and toes • A ophthalmologist and an otolaryngologist might be needed incase of a hearing and vision problem and other related issues • Other specialist will be needed as patient will require other services
Dental treatment: • Both patient and guardian should learn oral hygiene instruction • Electrical toothbrush should be recommended • Short intervals appointments for professional prophylaxis • Chlorhexidine mouth rinse 0.2% may be used twice a day for 2 weeks • Depending on the patients case, DDS may choose to extract teeth and use orthodontic appliances to provide normal occlusion • Topical fluoride is recommended as a preventative measure • DDS may refer patient to a reconstructive surgeon to fix abnormality in the extremities it will provide patient the ability to use hands
Resources: • http://ghr.nlm.nih.gov/condition/apert-syndrome • http://www.webmd.com/children/apert-syndrome-symptoms-treatments-prognosis • http://www.scielo.br/pdf/roc/v26n1/a21v26n1.pdf • http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/apert-syndrome/ • Images: • https://en.wikipedia.org/wiki/Apert_syndrome#/media/File:Patient_with_Apert_syndrome.jpg • http://www.facesplus.com/procedures/craniofacial/congenital-disorders/syndromic-craniosynostosis/ • http://www.pediatricsconsultant360.com/content/newborn-bicoronal-synostosis-and-syndactyly-hands-and-feet • http://imagelogr.com/i-sindrome-de-apert.php?adoff • http://escholarship.org/uc/item/95f8927g