Download
1 / 36
900 likes | 3.52k Views
ISCHEMIA & INFARCTION. Objectives. To learn ischemia and ischemic changes To be able to define infarction To learn types of infarcts. Ischemia. Failure of blood supply. Adequate blood circulation. Proper function of the heart, The integrity of the vasculature,

E N D
Objectives • Tolearnischemiaandischemicchanges • To be ableto define infarction • Tolearntypes of infarcts
Ischemia Failure of blood supply
Adequate blood circulation • Proper function of the heart, • The integrity of the vasculature, • The maintenance of a delicate balance between the coagulation and fibrinolytic systems.
Ischemia • Localized (leads to ischemic necrosis of tissue infarction) • arterial obstruction • deficient venous drainage, • Generalized ( leads to a generalized decrease in tissue perfusion shock) • severe decrease in cardiac output.
Etiology • Arterial obstruction • Atherosclerosis • Thrombosis • Thromboembolism • Venous obstruction • Thrombosis • Thromboembolism
Effect of Arterial Obstruction • Availability of Collateral Circulation. • Radial artery occlusion does not produce ischemia in the hand because the collateral ulnar artery circulation will compensate. • Obstruction of the end artery leads to complete cessation of blood flow and infarction (eg, the central artery of the retina or the middle cerebral artery).
Collateral Circulation • Integrity of Collateral Arteries • Atherosclerotic narrowing of thecollateral arteries in older people, • ischemia to the brain (when one internal carotid artery is occluded. • Rate of Development of Obstruction • Sudden arterial obstruction produces more severe ischemic changes than does gradual occlusion • sudden occlusion of a previously normal coronary artery leads to myocardial infarction.
Tissue Susceptibility to Ischemia • Brain and heart • infarction (ischemic necrosis) occurs within minutes • Tissue Metabolic Rate • Cooling • general decrease in the tissue's metabolic requirements • organs to be transported for transplantation.
Effect of Venous Obstruction • Venous obstruction • Large vein: Inadequate collateral drainage congestion edema, • Congestion and edema of the face when the superior vena cava is occluded (strangulation). • Acute severe venous congestion rise in hydrostatic pressure capillary rupture hemorrhage, • Orbital congestion and hemorrhage in cavernous sinus occlusion. • In extreme cases, venous infarction (red infarction) may result.
INFARCTION • Infarction: Tissue death caused by blockage of total blood flow (ischemia) • Infarct: Localized ischemic necrosis
Both parenchymal cells and interstitial tissue undergo ischemic necrosis(Infarction). • Infarction is most commonly due to the blockage of total blood flow • Arterial obstruction (thrombosis or embolism) • Venous obstruction. Partial occlusion may cause infarction, but more often leads to atropy (vascular atrophy).
Causes of Vascular Occlusion • (1) Occlusive thrombus and embolism(most common) • (2) Extramural compression • Fibrosis • Neoplasm, superior vena cava compression by a mediastinal tumor • (3) Diseases of the vessel wall • Atherosclerosis • Vasculitis • (4) Arterial spasm • Ischemia in the brain and myocardium (rare).
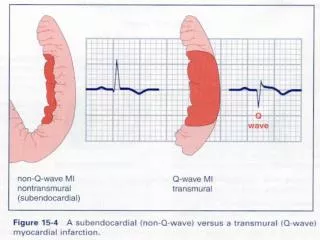
Classification of Infarcts • Pale(white, anemic) infarcts • Arterial obstruction in solid organs (heart, kidney, spleen), • No significant collateral circulation. • Red(hemorrhagic) infarcts • Double blood supply (eg, lung and liver), • Collateral vessels (intestine). • Associated with congestion and hemorrhage.
Sterile(aseptic) infarcts • Most infarcts are sterile. • Septic infarcts • Secodary bacterial infection of the necrotic tissue. • Septic infarcts occur: • (1) septic thromboembolism (emboli in acute infective endocarditis); • (2) when infarction occurs in a tissue (eg, intestine) that normally contains bacteria; • (3) bacteriemia (when bacteria from the bloodstream cause secondary infection). Septic infarcts are characterized by acute inflammation that frequently converts the infarct to an abscess.
Morphology of Arterial Infarctions • In kidney, spleen, and lung • wedge-shaped (conical), with the occluded artery situated near the apex of the wedge and the base of the infarct located on the surface of the organ. • In brain • Liquefaction cystic cavity. • Infarcts of small intestine • Occlusion of the superior mesenteric artery.
Myocardial infarcts • Irregular • Determined by the distribution of the occluded artery and the limits of collateral arterial supply • In patients with extensive collaterals, the infarcted area may be much smaller.
Morphology of Venous Infarctions • Total occlusion of all venous drainage • superior sagittal sinus thrombosis, • renal vein thrombosis, • superior mesenteric vein thrombosis. • Severe edema, congestion, hemorrhage, and a progressive increase in tissue hydrostatic pressure. • Increase in hydrostatic pressure obstruction of arterial blood flow ischemia infarction. • Always hemorrhagic (red infarct).
Special types of venous infarction: • Strangulation • Constriction of the neck of a hernial sac infarction of the contents of the sac, • Torsion • twisting of the pedicle of an organ (testis) venous obstruction hemorrhagic infarction.
Development of an Infarct (1) The nature of the vascular supply, (2) The rate of development of the occlusion, (3) The vulnerability of the tissue to hypoxia.
(1) The nature of the vascular supply • Most important factor • Dual arterial supply • Lungs (pulmonary and bronchial arteries) • Liver (hepatic artery and portal vein) • Hand or forearm (radial and ulnar arteries) • End-arteries • Kidneys • Spleen. • Acquired collateral circulation • Coronary arterial supply to the myocardium.
(2) The rate of development of the occlusion • Slowly developing occlusions are less likely to cause infarction. (3) The vulnerability of the tissue to hypoxia • Neurons • Myocardial cells • The epithelial cells of the proximal renal tubules.
Microscopical Evolution of Infarcts Myocardial infarct acute inflammatory response (congestion and neutrophil emigration) lysosomal enzymes lysis of the infarcted area (heterolysis) macrophages phagocytose the liquefied debris granulation tissue scar formation repair by scar contraction.
Cerebral infarct liquefaction (autolysis)abundant microglia phagocytose the debris (foamy cells) fluid-filled cystic cavity proliferation of reactive astrocytes gliosis.
Complete healing : • Vary with size. • A small infarct may heal within 1-2 weeks, • A larger one may take 6-8 weeks or longer. • Evaluation of the gross and microscopic changes in an infarcted area enables the pathologist to assess the age of an infarct, • Forensic Pathology: important consideration at autopsy in establishing the sequence of events that caused death.
THANK YOU FOR YOUR INTEREST