Download
1 / 26
270 likes | 573 Views
ACE Inhibitors. Randal A. Skidgel. From: Skidgel and Erdös , AHA Hypertension Primer, 2008. ACE Inhibitors. ACE = Angiotensin I Converting Enzyme 10 ACE inhibitors available in US:

E N D
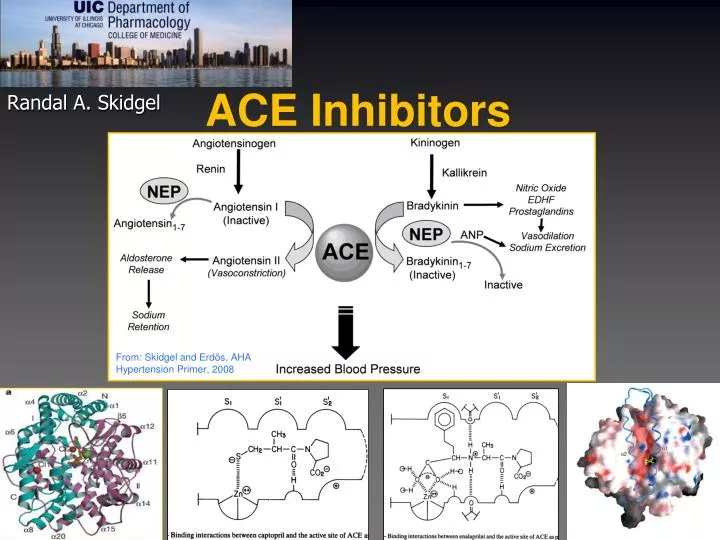
ACE Inhibitors Randal A. Skidgel From: Skidgel and Erdös, AHA Hypertension Primer, 2008
ACE Inhibitors • ACE = Angiotensin I Converting Enzyme • 10 ACE inhibitors available in US: • benazepril, captopril, enalapril, fosinopril, lisinopril, moexipril, perindopril, quinapril, ramipril and trandolapril. • ACE inhibitors were the 4th most prescribed drug class in the U.S (159.8 million Rx in 2008). • Lisinopril was the 2nd most prescribed drug in the US (75.5 million Rx in 2008).
The Renin-Angiotensin and Kallikrein-Kinin Systems From: Skidgel RA and Erdös EG, Hypertension Primer, 4th Edition, Chap. A15, 2008.
Scheme of Peptide Hormone Processing & Metabolism Receptor 1 RK RR Prohormone Endoprotease Processing Enzyme Active Peptide Peptidase 1 Peptidase 2 Receptor 2
Strategies for Developing Therapeutic Agents Receptor 1 Administer the Peptide Active Peptide Peptidase 1 Peptidase 2 Receptor 2
Use of Peptides as Drugs • Advantages • Highly potent/excellent specificity • Wide variety of Biological Activities • Straightforward Synthesis • Predictable Chemistry • Little or no toxicity from metabolism • Disadvantages • Oral administration difficult because of: • Degradation by digestive enzymes and intestinal peptidases • Poor absorption across tight junctions in epithelila • Efflux systems may pump absorbed peptides back out • Inconvenient administration • Rapidly cleaved by peptidases • Excreted by kidney • Relatively expensive to synthesize compared with small organic molecules
Strategies for Developing Therapeutic Agents Receptor 1 Block Degradation by Peptidases Peptidase 1 Peptidase 2 Receptor 2
Strategies for Developing Therapeutic Agents Use a Receptor Antagonist Active Peptide Peptidase 1 Peptidase 2 Receptor 1 Receptor 2
Strategies for Developing Therapeutic Agents Receptor 1 RK RR Prohormone Endoprotease Block Synthesis/Processing Processing Enzyme Active Peptide Peptidase 1 Peptidase 2 Receptor 2
ACE DISTRIBUTION • Widespread, concentrated on: • Endothelial surface of the vasculature • Epithelial Brush borders • Renal proximal tubules • Small intestine • Placenta • Choroid plexus ACE
Structure of Human Angiotensin Converting Enzyme (ACE) ACE N-domain ACE C-domain
A given peptidase can cleave a variety of peptides Example: Angiotensin Converting Enzyme (ACE)
ACE Inhibitors ACE AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Blood Pressure Mechanism of Action of ACE Inhibitors Angiotensinogen Kininogen Kallikrein Renin Kinin B2 Receptor Bradykinin Angiotensin I (Inactive) Angiotensin II Vasodilation Na+ Excretion Bradykinin(1-7) (Inactive)
ACE Mechanism of Action of ACE Inhibitors II Angiotensinogen ACE Inhibitors Renin Endopeptidases AT1-7/Mas Receptor Angiotensin 1-7 Angiotensin I (Inactive) Vasodilation Na+ Excretion Anti-inflammatory Oxidative stress Angiotensin II Angiotensin 1-5 (Inactive) AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Pro-inflammatory Oxidative stress Blood Pressure
Clinical Use of ACE Inhibitors • Antihypertensive • ~ 50% response (~90% with diuretic) • ↓Systemic Vascular Resistance • ↓Stress or Relfex induced sympathetic stimulation • → Heart rate • ↑ Sodium excretion, ↓ Blood volume • Congestive Heart Failure • ↓Vascular Resistance, Blood volume, Heart rate • ↑ C.O. (no change in myocardial O2 consumption) • Diabetic Nephropathy • Dilates afferent and efferent renal arterioles • ↓Glomerular capillary pressure • ↓Growth of mesangial cells/matrix due to Ang II?
Side Effects/Contraindications • Common • Dry Cough • 5 – 20% of patients • Not dose-related; occurs within 1 wk. – 6 mo. • Women > men • May Require cessation of therapy • Fetopathic Potential • Not teratogenic in 1st trimester • Developmental defects in 2nd or 3rd trimester • Rare • Angioneurotic Edema (or Angioedema) • ~0.1 - 0.5% of patients • Not dose-related; occurs within 1st week • Severe swelling of mouth, tongue, lips, airway • may be life-threatening
Side Effects/Contraindications • Rare • Hypotension • First dose effect in patients with elevated PRA, salt depletion, CHF • Hyperkalemia • In patients with renal insufficiency, diabetic nephropathy • Acute Renal Failure • Patients with renal stenosis, heart failure, volume depleted • Skin Rash • Extremely Rare (reversible) • Alteration/loss of taste • Neutropenia • Glycosuria • Hepatotoxicity
Drug Interactions • Antacids • May reduce bioavailability of ACE inhibitors • Capsaicin • May worsen ACE inhibitor-induced cough • NSAIDs • May reduce antihypertensive response to ACE inhibitors • K+-sparing Diuretics or K+ supplements • May exacerbate ACE inhibitor-induced hyperkalemia
Additional Beneficial Effects of ACE Inhibitors • Cardioprotective • Reduce incidence of second heart attack • Reduce cardiovascular complications in patients with risk factors • Reduce incidence of diabetes in high risk patients • Reduce complications in diabetic patients
Novel and Unexpected Functions of ACE and ACE inhibitors • ACE inhibitors induce protein crosstalk between ACE and bradykinin B2 receptor, enhancing signaling. • ACE inhibitors are direct agonists of the B1 kinin GPCR and induce endothelial nitric oxide production. • ACE inhibitor binding to ACE itself activates the MAP kinase JNK and stimulates gene transcription. See: Erdös EG, Tan F, and Skidgel RA. Angiotensin I-converting enzyme inhibitors are allosteric enhancers of kinin B1 and B2 receptor function. Hypertension 55: 214-220, 2010
Other antihypertensive drugs that interfere with the Renin-Angiotensin System Angiotensinogen Kininogen Kallikrein Renin B2 Receptor Bradykinin Angiotensin I (Inactive) ACE Angiotensin II Vasodilation Na+ Excretion Angiotensin Receptor Antagonists (the “sartans”, e.g. Losartan) Bradykinin(1-7) (Inactive) AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Blood Pressure
Other antihypertensive drugs that interfere with the Renin-Angiotensin System Angiotensinogen Kininogen Renin Inhibitor Aliskiren Kallikrein Renin B2 Receptor Bradykinin Angiotensin I (Inactive) ACE Angiotensin II Vasodilation Na+ Excretion Bradykinin(1-7) (Inactive) AT1 Receptor Vasoconstriction Aldosterone release Na+ Retention Blood Pressure