Download
1 / 39
1.22k likes | 3.81k Views
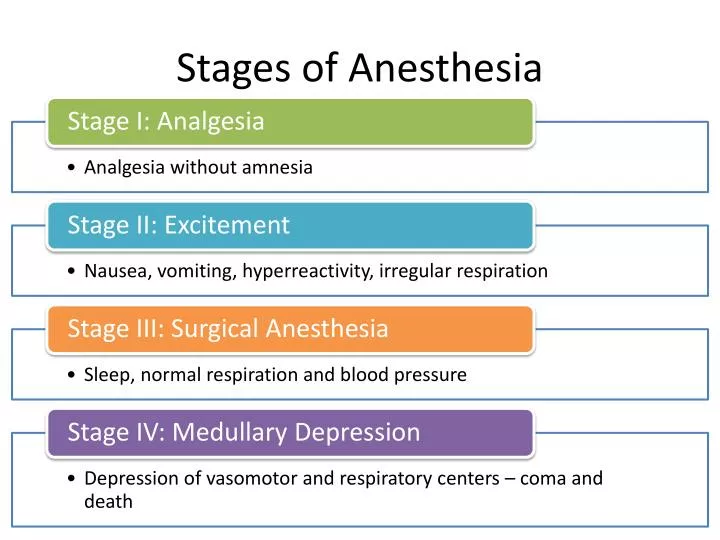
Stages of Anesthesia. What are common causes of periop cardiac arrest?. Anesthestic -related Cardiac Arrest and Its Mortality: A Report Covering 72,959 Anesthetics over 10 Years from a US Teaching Hospital. medication-related in 40%,

E N D
Anesthestic-related Cardiac Arrest and Its Mortality:A Report Covering 72,959 Anesthetics over 10 Years from a US Teaching Hospital • medication-related in 40%, • complications associated with central venous access in 20%, • airway-related complications in 20%, • unknown or possible vagal reaction in 13%, • and perioperative myocardial infarction in a single case Newland MC, Ellis SJ, Lydiatt CA, Peters KR, Tinker JH , Romberger DJ , Ullrich FA, Anderson JR (2002) Anesthesiology 97:108–15
Crisis management during anesthesia: cardiac arrest • ECG rhythm at the time of the arrest was reported in 86 cases (67%). • sinus bradycardia (23%) • asystole(22%) • Tach/v tach/v-fib (14%); • Pulseless electrical activity (7%) • 29 reports in which details of oxygen sat were included • 11 of the 29 were associated with hypoxaemia and the rest were associated with other causes, mostly direct drug effects and autonomic stimulation W B Runciman, R W Morris, L M Watterson, J A Williamson and A D Paix Qual. Saf. Health Care 2005;14;e14 doi:10.1136/qshc.2002.004473
Ventricular Fibrillation / Tachycardia • most common cause of sudden cardiac arrests • ends in death within minutes unless corrective measures are promptly taken. • useless quivering of heart no blood flow • Tx: only one therapy works defibrillation • Defibrillation success: chances drop every minute
Minutes: collapse to 1st shock Ventricular Fibrillation / Tachycardia • Survival reduced 7-10%/min (without CPR) • Rapid defibrillation is key • CPR prolongs VF, slows deterioration Eisemberg JAMA 1979; 241:1905-1907
Alpha Adrenoreceptor Review • a1 Receptors - Stimulation leads to Constriction of Vascular Smooth Muscle • Increases Peripheral Vascular Resistance (PVR). • a2 Receptors – Stimulation Inhibits NE Release
Beta Adrenoreceptor Review ß1 Receptors - Stimulation Results in Increased Heart Rate, Conduction Velocity and Contractility ß2 Receptors - Relaxation of Vascular Smooth Muscle, Skeletal Muscle and Bronchial Smooth Muscle
Epinephrine • Stimulates a and ß Adrenergic Receptors • Low Doses - ß Effects predominate • High doses, a effects predominate. • Increases Heart Rate, Increased Contractility. • Net Effect - Increase in Cardiac Output due to effect of ß1 Receptor • Constricts Arterioles of Skin, Mucous Membranes, and Viscera. • Net Effect – Increase in PVR due to effect of a1 Receptor
Epinephrine • Indications • Increases: • Heart rate • Force of contraction • Conduction velocity • Peripheral vasoconstriction • Bronchial dilation
Epinephrine • Dosing • 1 mg IV push; may repeat every 3 to 5 minutes • May use higher doses (0.2 mg/kg) if lower dose is not effective • Endotracheal Route • 2.0 to 2.5 mg diluted in10 mL normal saline
Epinephrine • Precautions • Raising blood pressure and increasing heart rate may cause myocardial ischemia, angina, and increased myocardial oxygen demand
Vasopressin • In Vivo – released from posterior pituitary in response to decreased ECF volume • Very powerful vasoconstrictor • Indications • Used to “clamp” down on vessels • No direct effects on heart
Vasopressin • Dosing • One time dose of 40 units only • May be substituted for epinephrine • If no response in 10-20 minutes resume epinephirne, do nor repeat doses of vasopressin • Not supported by human data • May be given down the endotracheal tube • DO NOT double the dose • Dilute in 10 mL of NS
Vasopressin • Precautions • May result in an initial increase in blood pressure immediately following return of pulse • Myocardial ischemia and angina • Increased peripheral vascular resistance
Antiarrhythmics • Interact with Electrolyte Channels in Atrial Muscle and/or Ventricular Muscle and/or SA Node and/or AV Node and/or Purkinjie Fibers • Class I – Sodium Channel Blockers: Procainamide, Lidocaine, Flecainide, Propafenone • Class II – ß Blockers • Class III – K Channel Blockers: Amiodarone, Sotalol, Ibutilide. • Class IV – Calcium Channel Blockers: Non Dihydropyridines. • Other – Adenosine, Digoxin, Magnesium Sulfate
Amiodarone • MOA: • delays repolarization (prolongs refractory period) • Blocks a and b adrenergic receptors • Affects sodium, potassium and calcium channels. • Indications • For refractory V Fib and Sustained V Tachycardia – Antiarrhythmic of 1st Choice • Powerful antiarrhythmic with substantial toxicity, especially in the long term
Amiodarone • Dosing • Should be diluted in 20 to 30 mL of D5W • 300 mg bolus after first Epinephrine dose • Repeat doses at 150 mg
Amiodarone • Precautions • May produce vasodilation & shock (hypotension, dizziness) • May have negative inotropic effects (bradycardia and heart block) • Terminal elimination • Half-life lasts up to 40 days
Lidocaine • MOA: • Depresses automaticity • Depresses excitability • Raises ventricular fibrillation threshold • Decreases ventricular irritability
Lidocaine • Dosing • Initial dose: 1.0 to 1.5 mg/kg IV • For refractory VF may repeat 1.0 to 1.5 mg/kg IV in 3 to 5 minutes; maximum total dose, 3 mg/kg • A single dose of 1.5 mg/kg IV in cardiac arrest is acceptable • Endotracheal administration: 2 to 2.5 mg/kg diluted in 10 mL of NS
Lidocaine • Precautions • Bradycardia, hypotension, heart block, sinus node depression
Magnesium Sulfate • Indications • Cardiac arrest associated with torsades de pointes or suspected hypomagnesemic state • Dosing • 1 to 2 g diluted in 10 mL of D5W IV push • Precautions • Occasional fall in blood pressure with rapid administration • Use with caution if renal failure is present
Asystole / Pulseless Electrical Activity • Asystole: lack of ventricular electrical activity & lack of ventricular mechanical activity • PEA: presence of organized ventricular electrical activity but not accompanied by meaningful ventricular mechanical activity (sufficient to generate a palpable pulse)
Acetylcholine Overview and Effects Heart – Decrease in Heart Rate by Reducing the Firing Rate of the SA node and Increasing Conduction Time through the AV node. Blood Vessels – Cause Mild Dilatation of Blood Vessels
Cholinergic Antagonists - Atropine • Atropine • Blocks Muscarinic Receptors – Post-Ganglionic Receptors in Parasympathetic Transmission • SA Node Effects - Increase Firing Rate • AV Node Effects – Decrease Conduction Time • Overall – Increased Heart Rate, Minimal BP Effect Reference: Grauer Page 78
Atropine Sulfate • Dosing • 1 mg IV push • Repeat every 3 to 5 minutes • May give via ET tube (2 to 2.5 mg) diluted in 10 mL of NS • Maximum Dose: 0.04 mg/kg
Atropine Sulfate • Precautions • Increases myocardial oxygen demand • May result in unwanted tachycardia or dysrhythmia
Tracheal administration of medications • Doses: 2 – 3 times iv dose • Dilute in 10cc distilled H2O or NS • N aloxone • Atropine • Vasopressin • Epinephrine • Lidocaine