Download
1 / 42
420 likes | 609 Views
Infant Mortality in Lane County. Using the Perinatal Periods of Risk Approach To Look at Local Fetal and Infant Mortality. Lane County, Oregon. Background Rural & urban population of 336,085 (4 th largest county in Oregon)

E N D
Infant Mortality in Lane County Using the Perinatal Periods of Risk Approach To Look at Local Fetal and Infant Mortality
Lane County, Oregon Background • Rural & urban population of 336,085 (4th largest county in Oregon) • Stretches from summit of Cascade Mountains to Pacific Ocean, 4,601 square miles • 60% live in Eugene/Springfield, 10% in small cities, 30% in rural areas • 80% of land is forested, half of that is federal land
Lane County, Oregon Population • 90.6% White • 0.8% Black/African American • 1.1% American Indian/Alaskan Native • 2.0% Asian • 0.2% Native Hawaiian/Pacific Islander • 1.9% other • 4.6% Latino of any race Population is Changing • Latino residents are very much “under-counted” • Minorities represent 10% of residents (Census) • Minority children in K-12 represent 20% of enrollment
The Problem • Lane County’s overall fetal-infant mortality rate is: ~Higher than the nation ~Higher than the state ~Higher than Multnomah, Clackamas, & Washington Counties (largest counties by population in OR) ~Higher than the Portland metropolitan area
“Infant mortality is the most sensitive index we possess of social justice” Julia Lathrop, Children’s Bureau, 1913
Why Perinatal Periods of Risk? Perinatal Periods of Risk (PPOR) is credible. • The PPOR approach has been used successfully by the Center for Disease Control (CDC) and other World Health Organization (WHO) collaborators to monitor and investigate fetal-infant mortality in developed and developing countries for many years.
Why Perinatal Periods of Risk? • PPOR is a simple, standardized approach that we can use locally to identify gaps and plan prevention activities • We can compare local fetal & infant mortality rates with that of other cities, counties, and states—as prepared by CDC and the March of Dimes
PPOR Steps 1. Bring community partners together 2. Map fetal & infant deaths 3. Focus on understanding the overall rate 4. Look for opportunity gaps 5. Target further investigations & prevention activities on gaps 6. Mobilize for sustainable systems change
Bring Community Partners Together Early Community Partnership Goals • Share initial fetal & infant mortality data with the community • Share PPOR approach • Begin discussion regarding the reasons for Lane County’s high infant mortality • Begin discussion on how we can work most effectively together to make a difference
Map Fetal & Infant Deaths Lane County Vital Stats Data 1. Fetal death files 2. Linked birth—infant death certificate files *Based on maternal residence at time of fetal death or live birth
Map of Local Data Includes Fetaland Infant Deaths (>24 weeks) Includes Very Low Birthweight(500-1,499 grams) & Higher Birthweight (>1,500 grams) Examinesbirthweight& AGE AT DEATH at the same time Generates a local “Map” for targeting strategic actions
1999-2003 PPOR Map Lane County Overall Fetal-Infant Mortality
1999-2003 PPOR Map Lane County Overall Fetal-Infant Mortality
Focus on understanding the overall rate • Lane County’s Overall Fetal-Infant Mortality Rate was 9.5 (1999-2003) • Fetal deaths at >24 weeks gestation & >500 grams; Infant deaths at > 500 grams. • 18,268 live births plus 66 fetal deaths (18,334) was the denominator for rate computation (1999-2003)
Map of Fetal-Infant Deaths Lane County 1999-2003 56/3.1 Maternal Health/ Prematurity (fetal deaths, live births) 43/2.3 Maternal Care (fetal deaths) 31/1.7 Newborn Care (live births) 44/2.4 Infant Health(live births) = 9.5 overall rate
Look for Gaps • All population groups, including the local reference group, had excessively high rates of fetal-infant mortality • Broad, over-reaching actions that impact all groups are needed • Numbers of deaths in rural areas, minority communities, and for moms aged 19 and under were inadequate for statistical analysis
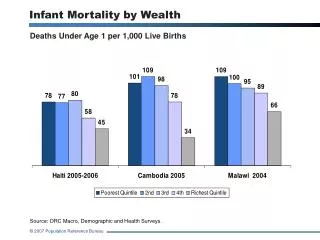
1999 – 2003 Lane County Fetal-Infant Mortality Rate by Group
Gaps in Lane County’s Map of Fetal-Infant Mortality • National PPOR reference group rate of 5.8 overall was used for comparison • Reference group (national and local) determined by maternal characteristics: age > 20 years, education > 13 years, White non-Hispanic • Excess rates of mortality and excess numbers of deaths were found in all four PPOR groups: maternal health/prematurity, maternal care, newborn care, and infant health
ExcessFetal-Infant Mortality Rates ____________________________________________________________
Lane County 1999-2003 Excess Fetal-Infant DeathsBased on US Reference Group
Target Further Investigations & Actions Investigations: Why the excess deaths? • Additional population-based data assessment & analysis • Individual fetal-infant case findings & analysis Actions: Based on PPOR group excess deaths • Infant health—safe sleep, breast feeding, injury prevention • Maternal health/prematurity—preconception health, health behaviors, perinatal care
Analyze AdditionalPopulation-Based Data • PRAMS (Pregnancy Risk Assessment Monitoring System) • Census data • Alcohol and Drug data • Mental Health data • Health care availability studies
PRAMS • County level data shows disturbing levels of alcohol and tobacco use. • One of four women admitted drinking more than 5 drinks at one sitting in the months immediately before (and therefore during the first months of) pregnancy; this was significantly higher than the state average • Tobacco use before and after pregnancy was also higher than the state average
PRAMS • Alcohol and tobacco use have been shown to be markers for illicit drug use • Lane County’s higher than expected levels of binge drinking and tobacco use indicate a high potential for co-occurring drug use
Vital Statistics Lane County’s fetal & infant death data was studied to identify: ~most frequent age range at time of death ~most frequent causes of death
Vital Statistics Age Range: • Data indicated that Lane County’s mortality rate for the postneonatal age range (29 days to 1 year) was statistically (significantly) higher than for Oregon as a whole
Vital Statistics Cause of Death: • Ill-defined causes of death (including SIDS and suffocation) accounted for 35.9% of postneonatal deaths and other external causes (accidents & injuries) accounted for 24.5% of postneonatal deaths—potentially preventable deaths (60.4%)
Census & Other Data • In 2005, Lane County had 3,487 births • Of the women who gave birth: ~34% were < 185% federal poverty level ~43% were first time parents ~35% were unmarried ~14% had < high school education
Census and Other Data • Over the past ten years, communities in Lane County have had large job losses in the timber industry and have struggled to establish an alternative economic base
Analyze individual case study data through Fetal Infant Mortality Review (FIMR) process • Infant death as a sentinel event • Multidisciplinary review team-health, social service, medical examiner • De-identified medical & social information • Maternal Interview
FIMR • Review information from individual cases of fetal & infant death in order to: • Identify factors associated with those deaths • Determine if those factors represent community-wide service system problems that require change • If so, to develop recommendations for change • Assist in the implementation of change
Mobilize for Sustainable Change • Large Community Group—Lane County Fetal-Infant Mortality Initiative meets quarterly • Workgroups on Data, Maternal health (preconception), and Infant Health meet monthly • Evidence based strategies are being examined to address identified areas of concern • Funding opportunities are being explored • Additional community mobilization continues through presentations, earned advertising
Next Steps • Update PPOR analysis with 2000-2004 data and yearly thereafter • Examine trends over time • Receive training in PRAMS data extraction, update complete PRAMS data • Continued resource development to sustain PPOR efforts & implement a FIMR
Lessons Learned • Initial efforts to inform and engage community were hampered by our lack of confidence about our ability to analyze & tackle the problem ~Enthusiasm & determination helped mitigate our lack of experience and confidence ~DaTA Institute provided much needed learning opportunities and support ~Support of Health & Human Services management was essential
Lessons Learned • Efforts were also hampered by the lack of dedicated FTE to the project—all of us just added more to our work load ~After first year, HHS loaned 0.15 FTE to coordinate meetings, take minutes, contact community members ~Budget for upcoming year (though not yet fully funded) includes staffing to keep efforts moving forward and to begin a FIMR
Lessons Learned • Efforts at fund raising were hampered by funder’s preference for non-governmental projects ~We keep writing grant proposals, have received acceptance of one & assurances for another ~We can now leverage the grant we have ~Presentations to local civic, business, & fraternal organizations increase awareness and help with fund raising
Infant Mortality is— “A sentinel event that serves as a measure of a community’s social and economic well-being as well as its health.” Buckley, K. A., et al., Fetal and Infant Mortality Review Manual: A Guide for Communities, 1998.
County Contacts • Dr. Sarah Hendrickson, Public Health Officer, PPOR Team Member, sarah.hendrickson@co.lane.or.us, 541.682.3956 • Karen Gillette, Public Health Manager, PPOR Team Member, karen.gillette@co.lane.or.us, 541.682.3950 • Pamela Stuver, Public Health Nursing Supervisor & PPOR Team Leader, pamela.stuver@co.lane.or.us, 541.682.4670 • Douglas Daniell, Management Analyst and PPOR Data Team Member, douglas.danielle@co.lane.or.us, 541.682.2047 • C.A. Baskerville, Sr. Program Services Coordinator, PPOR Team Member, cindy.baskerville@co.lane.or.us, 541.682.3031 • Sandy Moses, Health Educator, PPOR Team Member, sandy.moses@co.lane.or.us, 541.682.3652