Download
1 / 1
10 likes | 82 Views
136. 102. 15. 97. 3.4. 25. 0.9. Ca, Mg, Phos normal. T Protein: 9.0 Albumin: 4.1 T Bili: 0.8 AST: 18 ALT: 30 AP: 100. 13.1. 8.6. 284. 39.5. MCV 79. Right lobe sagittal. Left lobe sagittal. Bilateral lobe transverse. No. Yes. Neck Pain. RAIU. Symptoms.

E N D
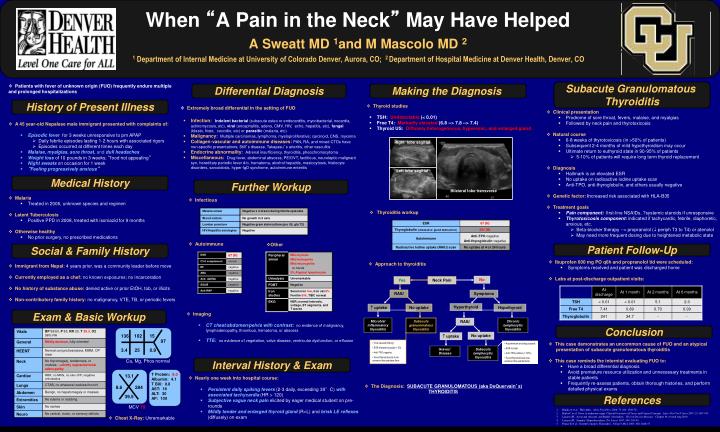
136 102 15 97 3.4 25 0.9 Ca, Mg, Phos normal T Protein: 9.0 Albumin: 4.1 T Bili: 0.8 AST: 18 ALT: 30 AP: 100 13.1 8.6 284 39.5 MCV 79 Right lobe sagittal Left lobe sagittal Bilateral lobe transverse No Yes Neck Pain RAIU Symptoms Hyperthyroid uptake No uptake Hypothyroid Microbial inflammatory thyroiditis Subacute granulomatous thyroiditis RAIU Chronic lymphocytic thyroiditis No uptake uptake • Viral caused (theory) • ESR elevated (usually > 50) • Anti-TPO negative • Fever/thyrotoxicosis more common than painless form • Autoimmune and drug caused • ESR normal • Anti-TPO positive (> 50%) • Fever/thyrotoxicosis less common than painful form Graves’ Disease Subacute lymphocytic thyroiditis When “A Pain in the Neck” May Have HelpedA Sweatt MD 1and M Mascolo MD 2 1 Department of Internal Medicine at University of Colorado Denver, Aurora, CO; 2 Department of Hospital Medicine at Denver Health, Denver, CO • Patients with fever of unknown origin (FUO) frequently endure multiple and prolonged hospitalizations Subacute Granulomatous Thyroiditis Differential Diagnosis Making the Diagnosis History of Present Illness • Thyroid studies • TSH: Undetectable (< 0.01) • Free T4: Markedly elevated (6.8 --> 7.8 --> 7.4) • Thyroid US: Diffusely heterogeneous, hyperemic, and enlarged gland • Thyroiditis workup • Extremely broad differential in the setting of FUO • Infection:Indolent bacterial (subacute osteo or endocarditis, mycobacterial, nocardia, actinomycosis, etc), viral (encephalitis, adeno, CMV, HIV, echo, hepatitis, etc), fungal (blasto, histo, coccidio, etc) or parasitic (malaria, etc) • Malignancy: Multiple carcinomas, lymphoma, myeloproliferative; carcinoid, CNS, myxoma • Collagen-vascular and autoimmune diseases: PAN, RA, and mixed CTDs have non-specific presentations; Still’s disease, Takayasu’s arteritis, other vasculitis • Endocrine abnormality: Adrenal insufficiency, thyroiditis, pheochromocytoma • Miscellaneous: Drug fever, abdominal abscess, PE/DVT, factitious, neuroleptic malignant syn, hereditary periodic fever d/o, hematoma, alcohol hepatitis, mastocytosis, histiocyte disorders, sarcoidosis, hyper-IgD syndrome, autoimmune enteritis • Clinical presentation • Prodrome of sore throat, fevers, malaise, and myalgias • Followed by neck pain and thyrotoxicosis • Natural course • 6-8 weeks of thyrotoxicosis (in >50% of patients) • Subsequent 2-4 months of mild hypothyroidism may occur • Ultimate return to euthyroid state in 90-95% of patients • 5-10% of patients will require long term thyroid replacement • Diagnosis • Hallmark is an elevated ESR • No uptake on radioactive iodine uptake scan • Anti-TPO, anti-thyroglobulin, and others usually negative • Genetic factor: Increased risk associated with HLA-B35 • Treatment goals • Pain component: first-line NSAIDs, ?systemic steroids if unresponsive • Thyrotoxicosis component: indicated if tachycardic, febrile, diaphoretic, anxious, etc. • Beta-blocker therapy --> propranolol ( periph T3 to T4) or atenolol • May need more frequent dosing due to heightened metabolic state • A 45 year-old Nepalese male immigrant presented with complaints of: • Episodic feverfor3 weeks unresponsive to prn APAP • Daily febrile episodes lasting 1-2 hours with associated rigors • Episodes occurred at different times each day • Malaise, myalgias, sore throat,and dull headaches • Weight lossof 10 pounds in 3 weeks; “food not appealing” • Night sweatson occasion for 1 week • “Feeling progressively anxious” Medical History Further Workup • Malaria • Treated in 2006, unknown species and regimen • Latent Tuberculosis • Positive PPD in 2008, treated with isoniazid for 9 months • Otherwise healthy • No prior surgery, no prescribed medications • Infectious • Other • Autoimmune Social & Family History Patient Follow-Up • Ibuprofen 600 mg PO q6h and propranolol tid were scheduled: • Symptoms resolved and patient was discharged home • Labs at post-discharge outpatient visits: • Approach to thyroiditis • Immigrant from Nepal: 4 years prior, was a community leader before move • Currently employed as a chef: no known exposures;no incarceration • No history of substance abuse: denied active or prior EtOH, tob, or illicits • Non-contributory family history: no malignancy, VTE, TB, or periodic fevers Exam & Basic Workup • Imaging • CT chest/abdomen/pelvis with contrast:no evidence of malignancy, lymphadenopathy, thrombus, hematoma, or abscess • TTE:no evidence of vegetation, valve disease, ventricular dysfunction, or effusion Conclusion • This case demonstrates an uncommon cause of FUO and an atypical • presentation of subacute granulomatous thyroiditis • This case reminds the internist evaluating FUO to: • Have a broad differential diagnosis • Avoid premature resource utilization and unnecessary treatments in stable patients • Frequently re-assess patients, obtain thorough histories, and perform detailed physical exams Interval History & Exam • Nearly one week into hospital course: • Persistent daily spiking fevers (2-3 daily, exceeding 39°C) with associatedtachycardia (HR > 120) • Subjective vague neck painelicited by eager medical student on pre-rounds • Mildly tender and enlarged thyroid gland (R>L) and brisk LE reflexes (diffusely) on exam • The Diagnosis: SUBACUTE GRANULOMATOUS (aka DeQuervain’s) • THYROIDITIS References Bindra A et al. Thyroiditis. Amer Fam Phys, 2006; 73 (10): 1769-76 Burke C et al. Fever of unknown origin: Clinical Overview of Classic and Current Concepts. Infect Dis Clin N Amer 2007; 21: 867-915 Lazarus JH. Acute and subacute, and Reidel’s thyroiditis. Thyroid Disease Manager. Chapter 19, revised Aug 2010 Lazarus JH. Seminar: Hyperthyroidism. The Lancet 1997; 349: 339-43 Pearce E et al. Current Concepts: Thyroiditis. N Engl J Med, 2003; 348: 2646-55 • Chest X-Ray: Unremarkable