Download

1 / 12
130 likes | 189 Views
Explore key arguments, types, and implications of user charges in health care financing. Learn about fixed and variable payment models, linear pricing, contextual factors, and limitations of cost sharing.

E N D
Financing Health Care SA407User Charges Wednesday, 21 October 2009 Faisal Latif Miranda Perra
Overview • Key arguments of user charges • Various types of user charges • Implications of applying user charges to different health care services
Fixed PaymentConsumer contributes a payment on receipt of a particular health service which is fixed independently of the quantity of goods or service consumedMC=0 except for the first unit
Variable Payment If the payment that the consumer makes varies with the quantity of a good or service consumed, this will be referred to as variable payment. X * C = VC X =number of units of a service or good consumed C =cost per unit
Linear Pricing S=p.c.x S=total payment p>0 =fractional share • Co-payment or user fee • Co-insurance • Fixed plus Linear (F+L) S=F+ p.c.x F=fixed element MP> P of the first unit • Two-part tariff
Non-linear (full marginal price (FMP)) • Insurance Deductibles or Excess MP=0 once insurance starts to cover the TC • Non-linear (partial marginal price (PMP)) • Balance billing MP< TC
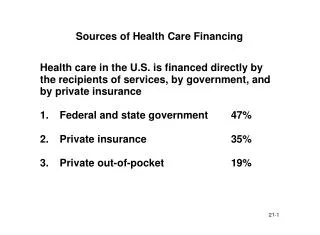
Contextual factors behind User Charges (Cost Sharing (CS) ) • Reasons cost sharing is employed • Instrument for promoting cost containment • Raising revenue • Contextual factors (country-specific) • Broad macroeconomic environment • Extent of population coverage (by a national health service) • Western Europe vs. CEE/CIS countries • Western Europe: minimal obligations for poorest individuals
Implications of User Charges (Cost Sharing) • Context: Rand Health Insurance Experiment (HIE) • Decreased utilisation of health services (Rice and Morrison, 1994) • ‘Necessary’ vs. ‘unnecessary’ utilisation • Rationale: reduce use of those services not ‘medically necessary’ • CS no selective effect (Lohr et al. 1986)
Implications of User Charges (Cost Sharing) • First Contact vs. Referral Services • Utilisation rate of primary care more sensitive to cost than referral services (more elastic) • Provider response • Providers will induce increase in intensity of referral care (due to decreased demand) • UMW Health & Retirement Fund • Introduction of co-payments • Physicians changed practice patterns to maintain income
Implications of User Charges (Cost Sharing) • Effect of CS on total health expenditure • CS does not ultimately contain costs • Why? Costs are primarily driven by supply-side factors • Paradox - lowest utilisation but highest HC expenditure – which country? Why? • Possible solution • Supply-side measures more effective mechanisms e.g. budgetary controls • Prescription drugs • Weak tool for cost-containment (Jönsson & Gerdtham, 1995).
Limitations of Cost Sharing (CS) • Information asymmetry • Heterogeneous health-service mix • Reduced equity in finance • Reduced equity in access & health status • Driven by supply-side • Policies required to address this • CS will only reduce utilisation, NOT cost containment • Considerable administration, information, economic and political constraints (Gilson et al., 1995)