Download
1 / 71
810 likes | 1.7k Views
Fever In Children. In the name of God. Fever. Fever Fever is a common symptom with various diseases in children Fever Definition A centrally mediated elevation of body temperature in response to stress or insult Rectal temperature is over 100.4°F (38°C) Oral temperature above 37.5°C

E N D
Fever In Children In the name of God
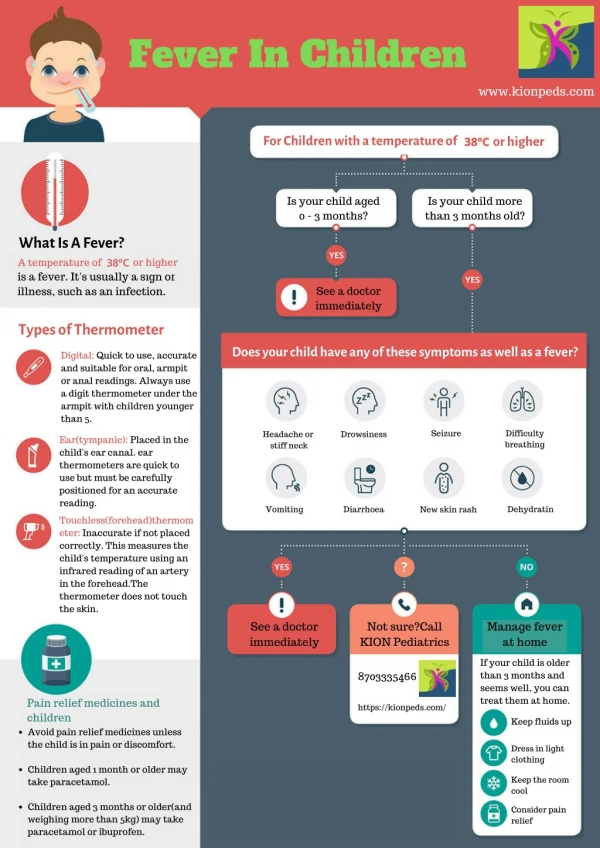
Fever Fever • Fever is a common symptom with various diseases in children Fever Definition • A centrally mediated elevation of body temperature in response to stress or insult • Rectal temperature is over 100.4°F (38°C) • Oral temperature above 37.5°C • Auxiliary temperature above 37.2°C
How to Take Oral (Mouth) Temperatures • Be sure a child has not had a cold or hot drink in the last 30 minutes. • Glass thermometer: • shake the thermometer until the mercury line is below 98.6°F (37°C) • Place the tip of the thermometer under one side of the tongue and toward the back ,not in front tongue. • Have your child hold the thermometer in place with his lips and fingers (not his teeth) • He should breathe through his nose, keeping his mouth closed. • Leave the glass thermometer in the mouth for 3 minutes. • see where the mercury line ends. Digital thermometer • turn it on. 2..4. Same as glass thermometer 5. Leave it in the mouth until you hear the correct signal (usually a series of beeps). 6. Read the temperature. • Fever is an oral temperature over 99.5°F (37.5°C).
How to Take Armpit (Axillary) Temperatures Glass thermometer • shake it until the mercury line is below 98.6°F (37°C). • Place the tip of the thermometer in a dry armpit. • Close the armpit by holding the elbow against the chest for 4 or 5 minutes. • After 4 or 5 minutes take it out and read the temperature by finding where the mercury line ends. Digital thermometer 1. turn it on 2..3. Same as glass thermometer 4. remove it after you hear the signal (usually a series of beeps) and read the temperature on the screen. Your child has a fever if the temperature is over 99°F (37.2°C). If you're not sure if it is correct, check it by taking a rectal temperature.
How to Take a Rectal Temperature Glass thermometer • shake until the mercury line is below 99°F (37.2°C). • Have your child lie stomach down on your lap. • Before you insert the thermometer, put some petroleum jelly on the end of the thermometer and on the anus. • Insert the thermometer gently into the bottom about 1 inch. If infant, gently insert the thermometer only 1/4 to 1/2 inch. Never try to force it past any resistance. Forcing could damage the bowel. • Hold your child still while the thermometer is in. • leave it in your child's bottom for 2 minutes before you take it out. • Read the temperature on the thermometer( see the end of the mercury line.) Digital thermometer • turn it on. 2..5. Same As glass thermometer • take it out when you hear the correct signal (usually a series of beeps). 7. Read the temperature on the thermometer If the rectal temperature is over 100.4°F (38°C), your child has a fever.
How to Take a Electronic Pacifier Temperature • Have your child suck on the pacifier until the temperature stops changing and you hear a beep. This usually takes 3 to 4 minutes. • Read the temperature. Your child has a fever if the pacifier temperature is over 100°F (37.8°C).
If your child has been outdoors on a cold day, he needs to be inside for 15 minutes before taking the temperature. (Earwax, ear infections and ear tubes, however, do not interfere with accurate readings.) Pull the ear backward to straighten the ear canal. Place the end of the thermometer into your child's ear canal and aim the probe toward the eye on the opposite side of the head. Then press the button. In about 20 seconds you can read the temperature. Your child has a fever if the ear temperature is over 100.4°F (38°C). How to Take an Ear Temperature
Feverin children • Fever is a controlled in body T overthe normal values for an individual • Body T is regulated by thermosensitive neuronslocated in the preoptic of anterior hypothalamomus • Termoregulatory responses include; increased or decreased sweating extracellular fluid volume regulation behavioral responses
Pathogenesis • Endogenous pyrogens including the : 1-cytokines interleukin 1and 6 2-TNF 3-INTERFERON • Exogenous pyrogens including the Microbes and microbial toxins which stimulate macrophages to produce endogenous pyrogens • Endotoxin can directly affec thermoregulation
Pathogenesis)con) • IncreaseT is associated with decrease microbial reproduction and increase inflammatory response • Fever may exacerbate ; cardiac insufficiency in heart disease or chronic anemia Pulmonary insufficiency in chronic lung disease Metabolic instability in diabetes mellitus or inborn error of metabolism
Heat illness • Situation in witch either environmental stress impair the ability of the central thermoregulatory mechanism to maintain normal body temperature or internal factors produce excessive heat or impair the body’s ability to dissipate metabolism heat • Body temperature is elevated despite a normal set-point in POAH
Example of Heat illness • Hyperthyroidism • Malignant hyperthermia • Anhidrotic ectodermal dysplasia • Pharmacologic agent • Medical drug (anticholinergics and phenothiazines) • Street drug
Fever is s friend or enemy? • Fever is a beneficial response in favor the host • Fever may directly impair reproduction or even the survival of an invading microorganism • Moderate fever may enhance the immunologic response
Fever is friend or enemy? • High fever can impair the immunologic response • Fever increase the basal metabolic rater by 10-12 % for 1 °C • Increase oxygen consumption • Carbon dioxide production • Increase Fluid and caloric requirements • can precipitate febrile seizures • May be associated with neurological manifestation irritability,delirium,disorientation and hallucinations
Treatment of Fever • Anti pyretic drugs should not proscribed routinely to febrile children • WHO recommend the use anti pyretic for children with fever of ≥ 39 C°
The decision to treat • when the patient is uncomfortable • susceptible To febrile seizure • Critically ill-sepsis or septic shock • Cardiac or respiratory failure • Neurological diseases or injury • Disturbed fluid ,electrolyte status
Acetaminophen • Is the first line therapy for childhood fever • Rapidly and almost completely absorb from GI • half-life in plasma about 2 hour • Dose 10-15 mg/kg/dose PO/PR Q 4-6 hr • Maximum 5 dose/24 hr
Acetaminophen Side affect • Skin rash and allergic reaction occasionally • Neuttropenia ,thrombocytopenia and pancytopenia rarely Toxic Effect • Hepatotoxicity • Renal tubular necrosis • Hypoglycemia coma
Acetaminophen • AAP recommend that rectal Acetaminophen therapy should be avoided unless specifically discussed with the health care provider and that direction be followed
Ibuprophen • Inhibit prostaglandin synthetase. • Dose 8-10 mg/kg Q 6-8hr Side affect • Gastiris • Gastrointestinal apset • Platelets aggregation
Acetaminophen versus Ibubrophen • Acetaminophen: • provided greater initial temperature reduction • Ibubrophen: • Provided more significant antipyretic effect at 4 hr • Temperature decrement lasted longer The two drug have equal tolerability
Nimesulide • A new NSAID is useful in treatment of fever • Was more effective than Acetaminophen for treatment of fever • Appear to be safe as Acetaminophen • Dose 1.5 mg/kg/Dose TID
Feverin children • Fever is a controlled in body T overthe normal values for an individual • Body T is regulated by thermosensitive neuronslocated in the preoptic of anterior hypothalamomus • Termoregulatory responses include; increased or decreased sweating extracellular fluid volume regulation behavioral responses
Pathogenesis • Endogenous pyrogens including the : 1-cytokines interleukin 1and 6 2-TNF 3-INTERFERON • Exogenous pyrogens including the Microbes and microbial toxins which stimulate macrophages to produce endogenous pyrogens • Endotoxin can directly affec thermoregulation
Pathogenesis)con) • IncreaseT is associated with decrease microbial reproduction and increase inflammatory response • Fever may exacerbate ; cardiac insufficiency in heart disease or chronic anemia Pulmonary insufficiency in chronic lung disease Metabolic instability in diabetes mellitus or inborn error of metabolism
Fever • Fever is a common manifestation of infectious disease but is not predictive of severity • Many infections are usually benign in normal hosts • Sepsis ,meningitis pneumonia ,osteoarticular infections , pyelonephritis may have significant morbidity or mortality • Most febrile episodes can be diagnosed by careful history and physical examination and few lab tests
Thecauses of fever • Infection • vaccines , • endocrine disorders, genetic disorders , metabolic disorders , immunologic and rheumatologic disorders • tissue injury, malignancy , drugs • granulomatous diseases , inflammatory diseases • factitious fever
Clinical Manifestation • Causes of very high T)>41) include : central fever , malignant hyperthermia drug fever , heatstroke • T lower than (<36) can be sepsis and more commonly with cold exposure , hypothyroidism , or overuse of antipyretic • Intermittent fever , sustained fever , Remittent fever , Relapsing fever , periodic fever
Type of fever • Intermittent fever - Fever that touches normal for a few hours during the day. It is seen in malaria, acute pyelonephritis, local boils and furuncles. tuberculosis, lymphoma, and juvenile rheumatoid arthritis (JRA) • Remittent fever - Fever that fluctuates between 1.5 degree F in 24 hours without touching normal. viral infections but also may occur with bacterial infections (especially endocarditis), sarcoid, lymphoma, and atrial myxoma. • Continuous fever - Fever that does not touch normal and fluctuates less than 1.5 degree F in a day. It is seen in enteric fever, Bacterial endocarditis, viral pneumonia. Typhoid fever, typhus, brucellosis, and many other infections
FeverProne to Relapse • Infectious causes • Noninfectious causes Behcet disease , crohn disease , SLE • Periodic fever syndromes: • familial Mediterranean fever • cyclic neutropenia • Hyper igD syndrome • (PFAPA) periodic fever aphthous stomatitis pharyngitis - adenopathy
Febrile Patients at increased Risk for Serious Baterial infections • Immunocompetentpatient: Neonates(28 days) infants<3 mo Infants and children 3-36 mo Hyperpyrexia(>40) Fever with petechiae Immunocompromised patients: Sickle cell disease -Asplenia Complement / properdin deficiency- Agammaglobulinemia AIDS – Malignancy Congenital heart disease Central venous line
Treatment • fever<39 in healthy children do not require treatment • Antipyretic therapy dose not change the course of infection • Antipyretic therapy is beneficial in high-risk patients • Hyperpyrxia indicates risk of; severe infection ,hypothalamic disorders ,CNS hemorrhage
Fever without localizing signs • usually acute onset present for< 1 wk. • Young infants limited signs of infection and difficult to distinguish between bacterial and viral infection.
Fever without localizing signs • Infants< 4 wk are at risk for; • late-onset bacterial diseases • Perinatally acquired herpes simplex virus • Acquire community pathogens
Infants<3mo with fever • Fever in this age should always suggest the possibility of serious bacterial disease • Pyelonephritis is more common in uncircumcised boys ,neonate and infants with UT anomalies and young girls • Other bacterial diseases include: • , pneumonia , omphalitis ,mastitis skin and soft tissue infection. otitis media
Infants<3mo with fever • Viral infection is identified in 70% • Bacteremia is present in 5% • Serious bacterial infection are present in 10-15% in T > 38
Approach to febrile infants <3 mo • Careful history and physical examination • Toxic infants must prompt hospitalizatIion and immediate parenteral antimicrobial therapy after B /C , U/C ,LP • Ceftriaxone 50- 80mg/day or cefotaxim 50mg/kg/dose and ampicillin 50/kg/dose. • If CSF IS abnormal vancomycin 15/kg/ dose should be given
Approach to febrile infant<3mo (con) 2-Infants with fever unlikely to have a serious bacterial infection if; • appear generally well and previously healthy • No evidence of skin, soft tissue, bone , joint and ear infection • Who have WBC5000-15000 and band <1500 * and U/A normal
Occult Bacteremia in children 3-36 m0 ¤* Occurs in 1.5% well appearing in this age with fever • Bacteremia is present in 11% pneumonia and • 1.5% otitis media or pharyngitis • S,pneumoniae , N,menigitidis and salmonella . • S,Pneumonia account for 90% of cases.