Download
1 / 21
330 likes | 778 Views
Red Blood Cell Permeability. Eric Duitsman Genevieve Roland. Plasma Membranes. As discussed in MCB 252, cells contain a phospholipid bilayer. It is amphipathic meaning it contains a hydrophilic and hydrophilic layer. Cells also contain internal plasma membranes. These membranes provide:

E N D
Red Blood Cell Permeability Eric Duitsman Genevieve Roland
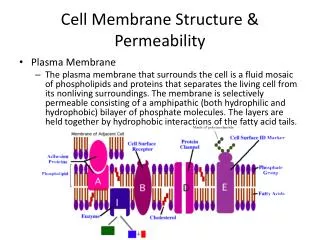
Plasma Membranes • As discussed in MCB 252, cells contain a phospholipid bilayer. It is amphipathic meaning it contains a hydrophilic and hydrophilic layer. Cells also contain internal plasma membranes. These membranes provide: • Transport of nutrients inward and waste outward via selective channels and pumps • They act as sensors that respond to external stimuli • They can increase in size without any loss of continuity simply by adding new membrane • They are flexible – they can expand and contract according to need • Within the membrane surfaces are regions called membrane domains • These are where proteins are localized which creates a specialized function
Osmosis • Osmosis is the term used for diffusion of water. This occurs only when two solutions are separated by a selectively permeable membrane. The water will move across the membrane in place of the solutes to create an equilibrium. • Osmolarity is osmoles/liter of the total solute concentration of a solution. • This also determines the concentration of water in a solution. • Water will move from an area of low to high osmolarity in order to reach an equilibrium • Osmolarity directly correlates with osmotic pressure • Osmotic pressure is the pressure required to act on a solution in order to prevent pure water from entering. • The greater the osmolarity, the greater the osmotic pressure. • The pressure depends on the number of particles in a solution
In an isosomotic cell, the total pressures of the two solutions are equal ao there is no movement across the membrane. An isoosmotic solution contains 300 mOsm of solute regardless of penetrating or not. Hyperosomotic condition is when the solution within a cell has a greater osmotic pressure than its surrounding environment. This solution contains more than 300 mOsm of solute. In a hypoosmotic state, the cell has less osmotic pressure than the solution in the extracellular zone. This solution contains less than 300 mOsm of solute in the cell.
Tonicity • The environment surrounding the cell and the effect that environment has on the cell is referred to as tonicity • This depends on the concentration of non-penetrating solutes in a solution. It does this while disregarding the penetrating solutes. • In a RBC, the volume is inversely related to the solute concentration in the extracellular medium. • In a hypotonic situation there is a lower concentration of non-penetrating solute in the extracellular fluid relative to the cell. This causes water to move into the cell and increase volume • In an isotonic situation there is an equal concentration • In a hypertonic situation there is a higher concentration causing water to move out and decrease volume
Urea • Urea is special in osmosis because it is able to rapidly diffuse across the cell membrane. This is opposite to glucose which diffuses much more slowly. A solution of 300 mOsm of NaCl and 100 mOsm urea has a 400mOsm/L osmolarity. This makes it hyperosmotic while still isotonic since the urea moves across the membrane to create an equilibrium between the cell and the extracellular fluid. This does not change the volume of the cell. • All hyposomotic solutions are also hypotonic however, a hyperosmotic solution can be hypertonic, isotonic, or hypotonic.
Blood • A blend of fluid (55%) and cells (45%) • Fluid consists of water, electrolytes, proteins, and nutrients • Three types of cells – red blood cells (~45%), white blood cells, and platelets (<1%) • The different cell types perform various tasks in the blood. • RBCs transport O2 and CO2 • They also deliver nutrients to all areas of the body. • Platelets form blood clots at wounds • White blood cells fight infections • Blood cells cannot reproduce as they do not contain a nucleus • Replaced by destroying old cells and creating new cells from the cells located in the bone marrow
Blood Types • Determined by blood types of parents • 4 different types • A, B, AB, and O • Antigens are found on the surfaces of the RBCs • These determine what the blood type is • All RBCs of a single individual have the same antigens on their surface
Antibodies (proteins) in the blood recognize antigens on the cell surface and bind to them. • Hemagglutination – agglutination of antibodies with the blood type antigens on RBCs • Anti-A will stick to A antigens resulting in hemagglutination. The same for Anti-B and B antigens. Blood Transfusions
Objectives • Be able to describe the effects and distinguish between hypotonicity and hypertonicity. • Distinguish between electrolytes and non-electrolytes • In regards to permeability • Demonstrate ability and mastery in slide preparation and use of a light microscope • Explain how the molecular weight of a substance can affect its permeability • Be able to explain the effects of polar groups on permeability • Summarize and illustrate permeability.
Part I – Effect of Electrolyte and Non-Electrolyte Concentrations on membrane Permeability • Materials • Gloves • 12 tubes • Sharpie • Tube Rack • NaCl • dH2O • Sucrose • Red blood cell suspension • Printed letter sheet • Slides equal to number of tubes whose contents remained intact and respective coverslips • P-200 • P-1000 • Light microscope
Procedure – Part I • Label your tubes 1-12 and place into the tube rack with #1-6 in the first rack and #7-12 in the second. NaCl used in 1-6 and sucrose, 6-12 • Using the chart given in the manual, determine amount of water and stock solution to combine to get desired NaCl and sucrose concentrations and add calculated amounts to respective tubes.
Part I - Continued • In quick succession, add 0.5 ml of the red blood cell suspension to tubes 1-12 using the P-1000. Make sure not to let the pipet tip touch the solutions in the tubes. • Cap the tubes and mix gently by swirling. • Set a timer for twenty minuets. At each five minute interval, hold the tubes against the printed letter sheet to see if hemolysis has occurred. If you compare the tube to the page and can see the letters through the solution, hemolysis has occurred. If the letters are not visible, the red blood cells are still intact.
Intact – non-hemolyzed Lysed - hemolyzed
Part I – Continued • After identifying the tubes in which hemolysis did not occur, label a slide with the corresponding number of those tubes. Place a 25 ul drop of the blood from these tubes on their respective slides using the P-200. Place a coverslip on the drop at an angle to reduce the amount of bubbles in the sample. Observe the slides under the microscope and determine the shape and size of the cells present from each solution. A slide with the original blood solution should also be made in order to compare any changes to. Crenated hypertonic Normal isotomic enlarged lysis hypotonic Osmolarity
Part II – The Effect of MW on Membrane Permeability • Materials • 0.3 M urea • 0.3 M ethylene glycol • 0.3 M glycerol • 0.3 M glucose • 4 tubes • P-1000 • Printed letter sheet
Procedure – Part II • Label tubes #1-4 and place into tube rack • Add 2 mls each to the respective tubes: • 1. 0.3 M urea – MW = 60 • 2. 0.3 M ethylene glycol - MW = 62 • 3. 0.3 M glycerol – MW = 92 • 4. 0.3 M glucose – MW = 180 • Add 0.5 ml of chilled blood into the tubes one at a time and time how long it takes for hemolysis to occur. Do this by holding against the printed page and record in seconds time elapsed • Record the times obtained for each substance and dispose of tubes in bleach tub
Part III – Blood Typing • Materials • Control ABO simulated blood samples • Tubes A, B, AB, O • Unknown blood samples of four patients • P1, D1, D2, D3 • Microtiter plate • Transfer pipets • Gloves • Toothpicks • Sharpie
Procedure – Part III • Place microtiter plate on a white piece of paper. • On cover of the plate, label the wells with the sample name using a sharpie A B AB O Anti-A Anti-B Donor 1 Donor 3 Patient Donor 2 Anti-A Anti-B
Part III - Continued • Plate 10 ul of each control blood type and patient sample into each of the corresponding labeled wells. Be sure to use a new transfer pipet for each sample. • Using a new pipet, add 10ul of anti-A serum into each of the 4 wells of the anti-A row. Repeat this for the bottom row • Do the same procedure with anti-B transferring into the 4 wells of the anti-B row in the top and bottom sections • Using a new toothpick for each sample, gently mix/stir the sample together • Allow plate to sit for 5-10 minuets • Observe the wells for the presence of agglutination. This occurs if the mixture has a granular texture rather than a smooth one. Record the results