Download
1 / 21
210 likes | 317 Views
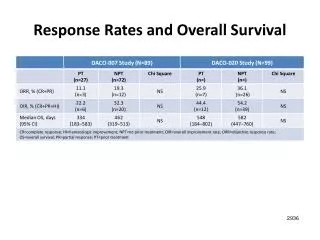
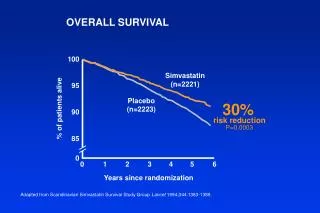
This analysis presents data from the Scandinavian Simvastatin Survival Study, highlighting the efficacy of Simvastatin in reducing overall mortality, coronary events, and hospitalizations. The study involved 4,444 participants and demonstrated significant risk reductions in overall survival (30%, P=0.0003) and coronary mortality (42%, P=0.00001) when compared to placebo. Additionally, major coronary event occurrence dropped by 34%, and myocardial infarction risk reduced by 37%. The findings emphasize Simvastatin's role in improving cardiovascular health and decreasing hospitalization days due to cardiovascular issues.

E N D
OVERALL SURVIVAL 100 95 90 85 0 Simvastatin(n=2221) Placebo(n=2223) % of patients alive 30% risk reduction P=0.0003 0 1 2 3 4 5 6 Years since randomization Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
CORONARY MORTALITY 200 150 100 50 0 189 No. of deaths 111 42% risk reduction P=0.00001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Kjekshus J et al Am J Cardiol 1995;76(9):64C-68C.
CAUSES OF MORTALITY 11.5% 8.2% Coronary Othercardiovascular Cancer Other Placebo(n=2223) Simvastatin(n=2221) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
MAJOR CORONARY EVENTS Coronary Death or Nonfatal MI 100 90 80 70 0 Simvastatin(n=2221) % of patients without events Placebo(n=2223) 34% risk reduction P <0.00001 0 1 2 3 4 5 6 Years since randomization Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
CORONARY EVENTS VS. BASELINE LDL Coronary Deaths or Nonfatal MIs by Baseline LDL-C Quartiles 40 35 30 25 20 15 10 5 0 36% 35% 33% 32% % risk reduction <4.39 mmol/L (170 mg/dl) 4.40–4.84 mmol/L (170–187 mg/dl) 4.85–5.34 mmol/L (188–207 mg/dl) >5.35 mmol/L (207 mg/dl) Baseline LDL-C Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1995;345(8960):1274-1275.
SUBGROUP COMPARISON –MAJOR CORONARY EVENTS Coronary Death and Nonfatal MI 33.4 35 30 25 20 15 10 5 0 29.5 Placebo Simvastatin 26.4 23.6 21.7 20.5 18.1 14.7 % of patients Men 34% risk reduction Women 34% risk reduction Age <65 34% risk reduction Age >65 34% risk reduction Adapted from Miettinen TA et al Circulation 1997;96:4211-4218.
CORONARY EVENT REDUCTION Simvastatinbetter Placebobetter Age Gender Smoking Hypertension Diabetes <60 yrs 60–70 yrs Men Women Yes No Yes No Yes No P <0.0001 P <0.0001 P <0.00001 P=0.01 P=0.00105 P=0.00009 P=0.00006 P <0.00001 P <0.00169 P <0.000001 0.2 0.4 0.6 0.8 1.0 1.2 Relative risk (95% Cl) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Kjekshus J et al Am J Cardiol 1995;76(9):64C-68C; Data on file, MSD.
MI REDUCTION Myocardial Infarction 600 500 400 300 200 100 0 562 369 No. of patients 37% risk reduction P <0.00001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Data on file, MSD.
NEED FOR PTCA/CABG 100 90 80 0 Simvastatin(n=2221) % of patients withoutPTCA or CABG 37% risk reduction P <0.00001 Placebo(n=2223) 0 1 2 3 4 5 6 Years since randomization PTCA = percutaneous transluminal coronary angioplasty; CABG = coronary artery bypass graft Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
HOSPITAL DAYS Cardiovascular Hospital Days 16,000 12,000 8000 4000 0 15,089 9951 No. of cardiovascularhospital days 34% reduction P <0.0001 Placebo(n=2223) Simvastatin(n=2221) Adapted from Pedersen TR et al Circulation 1996;93(10):1796-1802.
ATHEROSCLEROSIS • Coronary arteries • Carotid arteries • Femoral arteries Atherosclerosis is a widespread disease affecting all vascular beds including
STROKE/TIA 6 5 4 3 2 1 0 Placebo(n=2223) 28% risk reduction P=0.033 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
CAROTID BRUITS* 2.5 2.0 1.5 1.0 0.5 0 Placebo(n=2223) 48% risk reduction P=0.009 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
INTERMITTENT CLAUDICATION* New or Worsening Intermittent Claudication 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 Placebo(n=2223) 38% risk reduction P=0.008 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
ANGINA PECTORIS* New or Worsening Angina Pectoris 40 35 30 25 20 15 10 5 0 Placebo(n=2223) 26% risk reduction P<0.0001 % of patients Simvastatin(n=2221) 0 1 2 3 4 5 6 Years *A post-hoc analysis of 4S Adapted from Pedersen TR et al Am J Cardiol 1998;81:333-335.
DEVELOPMENT OF HEART FAILURE 100 98 96 94 92 90 0 Simvastatin(n=2221) % without CHF Placebo(n=2223) 21% risk reduction P <0.015 6 12 18 24 30 36 42 48 54 60 66 72 Months since randomization Adapted from Kjekshus J et al J Card Fail 1997;3(4):249-254.
CHOLESTEROL PARAMETERS Simvastatin 20 mg, Week 6 20 10 0 –10 –20 –30 –40 +8% P <0.0001 –15% Mean % change –28% –38% LDL-C Total C HDL-C Triglycerides Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Data on file, MSD.
PATIENT FOLLOW-UP Placebo Simvastatin (n=2223) (n=2221) Lost to follow-up 0% 0% Treatment discontinuations 13% 10% Adverse effects 6% 6% Personal reasons/other 7% 5% Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
TRANSAMINASES AND CK Elevations Occurring More than Once during 5.4 Years of Therapy Placebo Simvastatin No. (%) No. (%) AST >3 ULN 7 (0.3) 5 (0.2) ALT >3 ULN 12 (0.6) 14 (0.7) CK >10 ULN 0 0 AST = aspartate aminotransferase; ALT = alanine aminotransferase; CK = creatine kinase; ULN = upper limit of normal Adapted from Pedersen TR et al Arch Intern Med 1996;156:2085-2092.
CONCOMITANT CARDIOVASCULARTHERAPY – BASELINE Simvastatin Placebo 20–40 mg Drug Class/Therapy No. No. Aspirin 815 822 Beta blockers 1266 1258 Calcium antagonists 668 712 Isosorbide mono/dinitrate 727 684 Thiazides 138 151 Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389.
LONG-TERM SAFETY • Simvastatin had an excellent five-year safety profile • Adverse experiences similar to placebo • Only one reversible case of myopathy reported • Incidence of liver enzyme elevations similar to that of placebo • No interactions reported with beta blockers, calcium-channel blockers, aspirin, and thiazides • No increase in cancer overall or at any particular site • No previously unrecognized adverse effects observed 4S provided the largest and longest follow-up of patients treated with simvastatin (5.4 median years) Adapted from Pedersen TR et al Arch Intern Med 1996;156:2085-2092.