Download
1 / 38
460 likes | 1.33k Views
DENTAL PLAQUE. BY DR. MANISHA MISHRA. Dental Plaque Yellowish white soft, tenacious, amorphous material deposited on tooth surface Formation Adherent layer of mucinous material from saliva Colonisation of layers by diffusion of micro organisms

E N D
DENTAL PLAQUE BY DR. MANISHA MISHRA
Dental Plaque • Yellowish white soft, tenacious, amorphous material deposited on tooth surface Formation Adherent layer of mucinous material from saliva Colonisation of layers by diffusion of micro organisms w/n 48 hrs whole layers constitute of microorganisms
Plaque deposition occurs in interproximal surface of posterior teeth i.e,labial and gingivial for lower and labial and palatal for upper teeth. Types: • Supragingival • Infragingival Composition: • 70-90%-Microorganisms • 10-30%-Inorganic and Organic substances
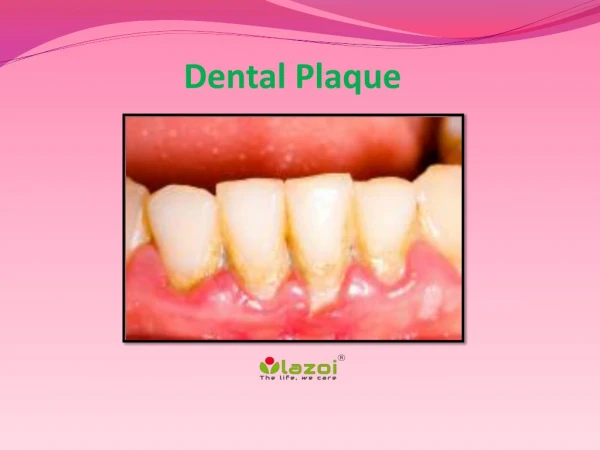
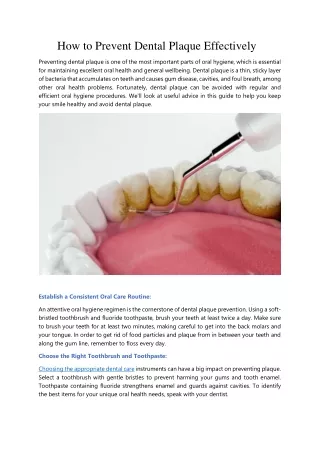
Dental Plaque Heavy staining and calculus deposits exhibited on the lingual surface of the mandibularanterior teeth, along the gumline.
Plaques initially populated by following: Organisms: • Gram positive Cocci/Bacilli • Gram negative Cocci and Bacilli • Fungus—Candida albican,Actinomycosisisraelli
1.Gram positive cocci— • Streptococcus-mutans,viridans,mitis,milleria,salivaris,pyogens,Staph- aureus,albus 2.Gram negative cocci— • NG,NM,NC 3.Gram positive bacilli— • Lactobacillus- acidiphilus,fermentation,odentolyticus 4.Gram negative bacilli— • H.influenzae,B.pertusis,Fusiform bacteria
Other than organisms: • Inorganic—Calcium,Sodium, Potassium,Phosphorus • Organic— Protein,Lipid, desquamated essential FA,Leucocytosis,Cells.
Growth of plaque • Multiplication of existing bacteria • Addition of new bacteria • Accumulation of metabolic products of bacteria • Food debris from diet Plaque leads to: • Acids released from dental plaque lead to demineralization of the adjacent tooth surface, and consequently to dental caries. • Saliva is also unable to penetrate the build-up of plaque and thus cannot act to neutralize the acid produced by the bacteria and remineralize the tooth surface. • They also cause irritation of the gums around the teeth that could lead to gingivitis, periodontal disease and tooth loss. • Plaque build up can also become mineralized and form calculus (tartar).
DENTAL PLAQUE Inadequate removal of plaque caused a build up of calculus (dark yellow color) near the gums on almost all the teeth.
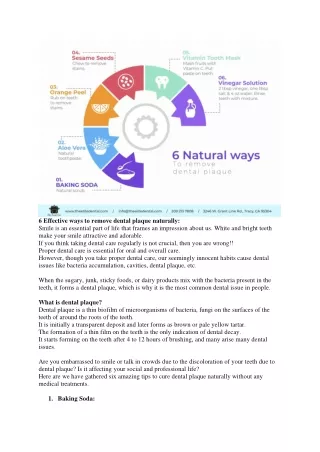
Prevention 1. Mechanical – Brushing , Flossing • Brush your teeth twice daily using a fluoride-based toothpaste. • Floss your teeth daily, or use an interdental cleaner. 2. Chemical – Mouth wash 3. Food intake – • Coarse, Dry (Avoid 3s sweet, sticky, soft) • Eat a balanced diet. • Avoid using tobacco products. • Limit the number of snacks you eat throughout the day. 4.Gingival massage
Dental Calculus (TARTAR) • Hard deposit formed on the tooth (due to mineralisation of dental plaque) • Plaque converted to calculus in 50 – 60 days Classification • Supragingival – coronal to gingival margin • Subgingival – below the crest of gingival margin
Supragingival calculus: • Colour=Yellowish to white ,Blackish • Consistency=clay like • Maximum occurs in Upper buccal region of molar teeth,lingual and interproximal surface of lower to anterior teeth. Subgingival calculus: • Dense brown to greyish black in colour
Composition: • 70-90%=Inorganic material • 10-30%=Organic material • Calculus formation can result in a number of clinical manifestations: • including bad breath • receding gums and • chronically inflamed gingiva.
Prevention • As in Plaque (oral hygiene) Treatment • Scaling 1. Manual and 2. Ultrasonic scaling
Dental caries • Irreversible progressive bacterial damage to the hard structures of the tooth characterised by demineralization resulting in the formation of a cavity Etiology --Decalcification by bacterial acid followed by destruction of all other tooth tissue • No theory is universally accepted • Acidogenic theory • Proteolysis chelation theory • Proteolytic theory
Acidogenic theory Dental caries is a sugar-dependent infectious disease. • Acid is produced from metabolism of carbohydrate by plaque bacteria, which results in a drop in pH at the tooth surface. • In response, calcium and phosphate ions diffuse out of enamel, resulting in demineralization. • This process is reversed when the pH rises again. • Caries is therefore a dynamic process characterized by episodic demineralization and remineralization occurring over time. • If destruction predominates, disintegration of the mineral component will occur, leading to cavitation.
Proteolytic theory • In addition to acid, proteolytic substances produced by plaque bacteria breakdown the organic portion of enamel and dentine
Proteolysis Chelation theory • Bacterial attack on enamel is initiated by keratinolytic bacteria causing breakdown of enamel protein • Organic and inorganic portion of enamel undergoes demineralization by formation of chelates
Saliva and caries • Saliva acts as an intra-oral antacid, due to its alkali pH at high flow-rates and buffering capacity. • In addition saliva: • ⇓ plaque accumulation and aids clearance of foodstuffs. • Acts as a reservoir of calcium, phosphate, and fluoride ions, thereby favouringremineralization. • Has an antibacterial action because of its IgA, lysozyme, lactoferritin, and lactoperoxidasecontent.
CARIOGENIC BACTERIA: • Streptococcus mutans • Streptococcus viridans • S. salivaries • S. mitis • S. sanguis • Lactobacillus
Properties of bacteria • Ability to produce acid by fermentation of sugars • Ability to polymerise sugars into long chain polysaccharides which make • plaque adhere firmly to the tooth surface and • Bacteria to one another • Lactic acid (main) and other is acetic acid
Prerequisites for development of dental caries • Dental plaque containing cariogenic bacteria • Bacterial substrate: sugar • Susceptible tooth surface • If pH < 5 then demineralization occurs
Enamel caries • The initial lesion is visible as a white spot. This appearance is due to demineralization of the prisms in a sub-surface layer, with the surface enamel remaining more mineralized. • With continued acid attack the surface changes from being smooth to rough, and may become stained. • As the lesion progresses, pitting and eventually cavitation occur.
DENTINE CARIES: • Dentine caries comprises demineralization followed by bacterial invasion, • but differs from enamel caries in the production of secondary dentine and the proximity of the pulp.
Diagnosis Early diagnosis is important Good eyesight (and a clean, dry, well-illuminated tooth) • Whitish or blackish spots • Cavity
Investigation • radiographs are useful in the detection of occlusal caries.
Management If lesion confined to enamel , institute preventive measures and keep under review. If lesion has penetrated dentine radiographically, a restoration is indicated unless serial radiographs show that it is static. • Removal of diseased enamel and dentine • Removal of pits and fissures • Restoration by filling • Posterior teeth • Cement & silver amalgam • Anterior teeth • Acid etch technique • RCT –Root canal treatment
Criteria for restoration: • Restoration should be watertight • Form of the tooth should be maintained so that occlusion is normal • Pulp should be protected with insulating cement lining
Prevention • Maintenance of oral hygiene • Proper brushing • Regular scaling • Avoid soft, sticky and sweet diet • Reduce bacterial load • Mouthwash with 0.2% chlorhexidine, betadine • Denial of substrate to plaque bacteria • Use saccharine( an artificial sweetener) as bacteria cannot utilize it • Complete removal of plaque by dentist • Scaling
Fluoride addition • Inhibits demineralization and promotes remineralization of early caries. • Fluoride enhances the degree and speed of remineralization and renders the remineralized enamel more resistant to subsequent attack. • Decreases acid production in plaque by inhibiting glycolysis in cariogenic bacteria. • An ⇑ concentration of fluoride in plaque inhibits the synthesis of extracellular polysaccharide.
Systemic fluoride • Water fluoridation in a concentration of 1 ppm (1 mg F /litre) gives a caries reduction of 50%. • Fluoride tablets • depends upon drinking water content • 1 tab contains 2.2 mg of Na Fluoride • <2 yrs : half tab • 2-12 yrs: 1 tab • > 12 yrs: half tab
Milk with 2.5-7 ppm F has been tried successfully. • Salt is cheap and effective for rural communities in developing countries where water fluoridation is not feasible
Fluorosis (or mottling) occurs due to a long-term excess of fluoride. • It is endemic in areas with a high level of fluoride occurring naturally in the water. • Clinically, it can vary from faint white opacities to severe pitting and discoloration.