Download
1 / 5
50 likes | 132 Views
AHA 2012. American Guidelines for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease. Key points.

E N D
AHA 2012 American Guidelines for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease Keypoints Fihn SD, Gardin JM, Abrams J, et al; American College of Cardiology Foundation/American Heart Association Task Force. Circulation. 2012;726(25):e354-e471. doi: 10.1161/CIR.0b013e318277d6a0.
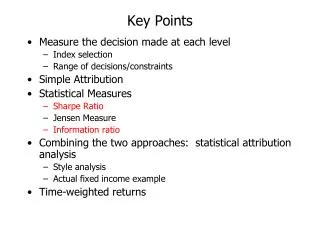
Medical therapy for relief of symptoms Class I, Level of evidence: B Class I, Level of evidence: B Class IIa, Level of evidence: B/A Add/substitute ranolazine Fihn SD, Gardin JM, Abrams J, et al; American College of Cardiology Foundation/American Heart Association Task Force. Circulation. 2012;726(25):e354-e471. doi:10.1161/CIR.0b013e318277d6a0.
Medical therapy for relief of symptoms • The management of stable CAD starts with lifestyle intervention. • Medical therapy is the first-line treatment for patients with stable CAD. • -Blockers are recommended as the initial treatment for relief of symptoms in patients with stable CAD. • If symptoms persist after medical therapy, physicians are advised to consider coronary artery revascularization. Fihn SD, Gardin JM, Abrams J, et al; American College of Cardiology Foundation/American Heart Association Task Force. Circulation. 2012;726(25):e354-e471. doi:10.1161/CIR.0b013e318277d6a0.
Therapy to prevent MI and death • Aspirin(class I, level of evidence: A) • -Blockers • For 3 years, in patients with normal LV function after MI or ACS • (class I, level of evidence: B). • In patients with LV systolic dysfunction (ejection fraction <40%) with heart failure or prior MI, unless contraindicated (carvedilol, metoprolol succinate, or bisoprolol) (class I, level of evidence: A). • For all other patients,-blockers are recommended (class IIb, level of evidence: C). • Renin-angiotensin-aldosterone system blockers • In patients with HT, diabetes mellitus, LV ejection fraction ≤40%, or chronic kidney disease, unless contraindicated(class I, level of evidence: A) or in patients with CAD and other vascular disease (class I, level of evidence: B). • ARBs are recommended in case of intolerability of ACE inhibitors(level of evidence: A). Fihn SD, Gardin JM, Abrams J, et al; American College of Cardiology Foundation/American Heart Association Task Force. Circulation. 2012;726(25):e354-e471. doi:10.1161/CIR.0b013e318277d6a0.
Antianginal agents not available in the United States • Ivabradine, nicorandil, trimetazidine. • In regard to trimetazidine, guidelines highlight: • The metabolic mode of action. • The clinical efficacy on ischemia and angina. • The anti-ischemic effects not associated with changes in heart rate or systolic blood pressure. • The data on cardiovascular end points, mortality, and quality of life. • The good tolerability. => Trimetazidine is not available in the United States, but is available in Europe and in more than 80 countries worldwide. Fihn SD, Gardin JM, Abrams J, et al; American College of Cardiology Foundation/American Heart Association Task Force. Circulation. 2012;726(25):e354-e471. doi:10.1161/CIR.0b013e318277d6a0.