Download

1 / 29
520 likes | 803 Views
Septic arthritis. http://hastaneciyiz. blogspot .com. Medical ppt. septic arthritis is an inflammatory joint disease caused by bacterial, viral, and fungal infection. Route of infection. dissemination of pathogens via the blood, from distant site…. (most common)

E N D
Septic arthritis http://hastaneciyiz.blogspot.com Medicalppt
septic arthritis • is an inflammatory joint disease caused by bacterial, viral, and fungal infection.
Route of infection • dissemination of pathogens via the blood, from distant site…. (most common) • dissemination from an acute osteomylitic focus • dissemination from adjacent soft tissue infection, • entry via penetrating trauma • entry via iatrogenic means
Etiology • The causal organism is usually Staphylococcus aureus. • In children under the age of 3 years Haemophilus influenzae is fairly common • gram-negative bacilli (a group of bacteria, including Escherichia coli, or E. coli) • streptococci (a group of bacteria that can lead to a wide variety of diseases)
Pathology • There is an acute synovitis with a purulent joint effusion and Synovial membrane becomes edematous, swollen and hyperemic, and produces increase amount of cloudy exudates contains leukocytes and bacteria • As infection spread through the joint, articular cartilage is destroyed by bacterial and cellular enzymes. • If the infection is not arrested the cartilage may be completely destroyed. • Pus may burst out of the joint to form abscesses and sinuses. • The joint may be become pathologically dislocated.
With healing there will be: • Complete resolution and return to normal. • Partial loss of cartilage and fibrosis. • Bone ankylosis • Bone destruction and permanent deformity.
Clinical presentation • Typical featuresare acute pain and swelling in a single large joint ,commonly the hip in children and the knee in adults, however any joint can be affected. • The most commonly involved joint is the knee (50% of cases), followed by the hip (20%), shoulder (8%), ankle (7%), and wrists (7%). interphalangeal, sternoclavicular, and sacroiliac joints each make up 1-4% of cases.
Symptoms in newborns or infants: • The emphasis is on septicemia rather than joint pain. • Irritability ,Fever, refuses to feed, rapid pulse. • Unable to move the limb with the infected joint (pseudoparalysis) . • Cries when infected joint is moved (diaper changing) • Infection is usually suspected ,but it could be anywhere so the joints should be carefully felt and moved to elicit the local signs of warmth ,tenderness and resistance to movement. • Umbilical cord or the site of injection should be examined for possible source of infection. • If the baby is distressed and wont move his/her leg think of hip infection.
In children: • Acute pain in single large joint. • The joint is swollen (if superficial), warm and tender. • Fever. • All movements are restricted due to muscle spasm (Pseudoparesis).
In adult: • Intense joint pain . • Joint swelling . • Joint redness . • Unable to move the limb with the infected joint . • Low-grade fever.
Physical examination • Decreased or absent rang of motion. • Signs of inflammation: joint swelling, warmth, tenderness and erythema. • Joint orientation as to minimize pain (position of comfort): • Hip: abducted, flexed and externally rotated. • Knee, ankle and elbow: partially flexed. • Shoulder: abducted and internally rotated
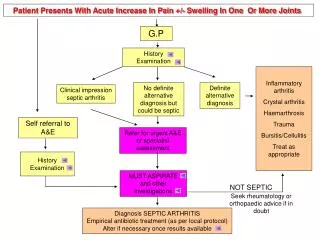
Investigation Lab studies: • The diagnosis can usually be confirmed by joint aspiration and immediate microbiological investigation of the fluid. • Blood culture may be positive in about 50% of proven cases. • Non specific features of acute inflammation-leucocytosis,ESR,CRP-are suggestive but not diagnostic .
Ask for: gram stain, culture, leukocyte count with differential, and crystal examination • leukocyte count: • generally higher than 50,000/µL, with a predominance of neutrophils more than 75% gram stain: • are positive in approximately 75% of patients with staphylococcal infections; however, results are positive in only 50% of patients with gram-negative infections
crystal examination: • exclude crystal-induced arthritis (may coexist) • culture: • The definitive method • for aerobic and anaerobic organisms. • are positive in 85-95% • Synovial fluid glucose, protein, and lactic acid concentration not specific.
Imaging studies 1-Plain x-ray: • The appearance of significant x-ray findings depends upon the duration and virulence of infection. • Plain radiography findings are generally nonspecific and may reveal only soft tissue swelling ,widening of the joint space ( due to the effusion), and periarticular osteoporosis during the first 2 weeks. • Later ,when the articular cartilage is attacked ,the joint space is narrowed.(persistent subluxation, destructive arthritis).
Septic arthritis of the hip following group B strep psoas abscess
2-Ultrasonography • This study is very sensitive in detecting joint effusions generated by septic arthritis. • Ultrasound can be used to define the extent of septic arthritis and help guide treatment. • Ultrasound helps to differentiate septic arthritis from other conditions (e.g., soft tissue abscesses, tenosynovitis) in which treatment may differ.
3-Radio-isotope bone scan: • Show increase uptake of the isotope in the region of the joint. (may help in difficult site as sacroiliac & sternoclavicular joints 4- CT scan: • This study may help to diagnose sternoclavicular or sacroiliac joint infections. 5-MRI: • MRI is most useful in assessing the presence of periarticular osteomyelitis as a causative mechanism.
DIFFERENTIAL DIAGNOSIS • Osteomyelitis: near a joint may be indistinguishable from septic arthritis ;the safest is to assume that both are present. • An acute haemarthrosis :either post-traumatic or due to a haemophilic bleed ,can closely resemble infection. The history is helpful and joint aspiration will resolve any doubt. • Transient synovitis(irritable joint) in children: causes symptoms and signs which are less acute ,but there is always the that this is the beginning of an infection. • Gout and pseudogout in adults :aspirated fluid may look turbid but the presence of urate or pyrophosphate crystals will confirm the diagnosis. • Rheumatic fever
complication • Dislocation: a tense effusion may cause dislocation • Epiphyseal destruction: in neglected infants the largely cartilaginous epiphysis may be destroyed ,leaving an unstable pseudarthrosis. • Growth disturbance: physeal damage may result in shortening or deformity • Ankylosis: if articular cartilage is eroded healing may lead to ankylosis • Secondary osteoarthritis • Osteomyleitis/abcess/sinus
Treatment • General Measures: The first priority is to aspirate the joint and examine the fluid, treatment is then started without further delay. • Analgesics and splinting of the involved joint in the position of maximal comfort alleviate pain. • Fluid replacement and nutritional support may be required. • Other foci of infection and any coexisting medical conditions must be identified and treated appropriately.
Intravenous antibiotics should be given empirically and started as soon as joint fluid and blood sample have been taken for culture. • If gram –positive organisms are identified ,Flucloxacillin is suitable . If in doubt ,a third generation cephalosporin will cover both game+ and gram- organisms. • Children less than 4 yr( if suspicion of H.Infl) treated with Ampicillin. • Once the bacterial sensitivity is known the appropriate drug is substituted. • Intravenous administration is continued for several weeks and is followed by oral antibiotics for a further 2 or 3 weeks.
Drainage: Indication of Surgical Drainage: 1-Joints that do not respond to antimicrobial therapy and daily arthrocentesis 2-. Any joint with limited accessibility, including the sternoclavicular or the hip joint 3-Patients with underlying disease, including diabetes, rheumatoid arthritis, immunosuppression, or other systemic symptoms, should be treated more aggressively with earlier surgical intervention
Thank you http://hastaneciyiz.blogspot.com Medicalppt