Download
1 / 33
990 likes | 3.22k Views
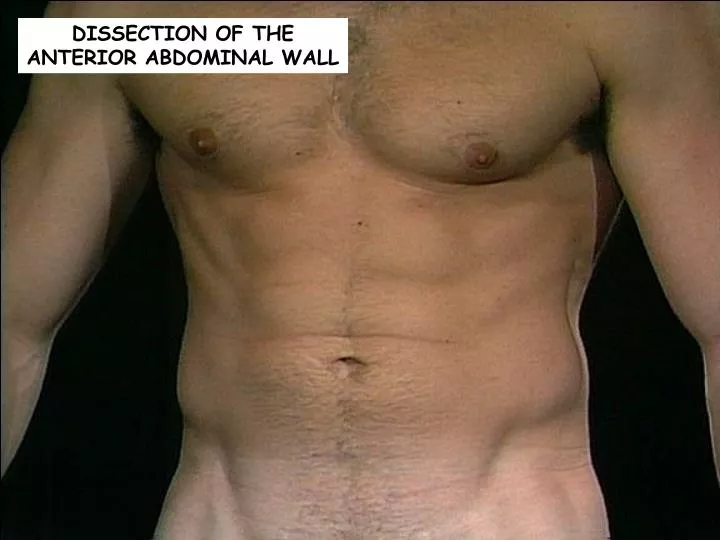
DISSECTION OF THE ANTERIOR ABDOMINAL WALL. Make a vertical midline incision through the skin from the xiphoid process to the pubic symphysis. (Be careful not to cut through the superficial fascia.)

E N D
Make a vertical midline incision through the skin from the xiphoid process to the pubic symphysis. (Be careful not to cut through the superficial fascia.) Then, make the a transverse incision from the superior end of the vertical incision to the midaxillary line bilaterally. From the inferior end of the vertical incision, cut along both pubic crests. Extend the incisions below the inguinal ligament along the iliac crest to the ASIS.
Once you have reflected the skin, but before removing the superficial fascia of the anterior abdominal wall, you may be able to identify some superficial epigastric vessels. These vessels may become engorged in individuals whose venous blood cannot freely return to the hear (such as obstruction of the hepatic portal vein) – and the patient will be said to have caput medusae.
Recall that the head of Medusa had writhing snakes for hair. In portal hypertension, blood "finds" alternative pathways back to the heart that do not pass through the liver. An uncommon path utilizes the umbilical vein, which directs blood through dilated superficial veins in the abdominal wall. These are visible on inspection of the abdomen and are known as caput medusae. http://www.smbs.buffalo.edu/pth600/IMC-Path/y1case/y1ans15.htm
Within the superficial fascia will be found different amounts of fat in different cadavers. (Yep, some of this fat may be removed via liposuction.) Make incisions through the superficial fascia at similar locations to those in the skin and reflect this fascia laterally. The superficial fascia is composed of two layers, the fatty outer layer, known as Camper’s fascia, and the more membranous inner layer, known as the Scarpa’s fascia, most prominent in the lower aspect of the abdominal wall below the level of the umbilicus.
Scarpa's fascia ends inferior to the inguinal ligament fusing with the fascia lata (deep fascia) of the thigh. In the midline, just superior to the penis, Scarpa's fascia contributes to formation of the fundiform ligament of the penis.
At this time, you should be able to observe several sites where anterior cutaneous nerves (terminations of ventral rami T7 – T12, which you will recall do NOT participate in the formation of any pleuxes) piercing the deep investing fascia lateral to the linea alba.
You may also see the iliohypogastric nerve, which is one of the terminal branches of L1. It provides sensation to the approximate region shown. It also provides motor input to the internal oblique and transversus abdominus mm..
You may also see the ilioinguinal nerve, which is the other terminal branch of L1. It provides sensation to the approximate region shown. It also provides motor input to the internal oblique and transversus abdominus mm..
Identify the linea alba that runs vertically from the xiphoid process to the pubic symphysis. The umbilicus generally lies at a midpoint in the linea alba. At the linea alba, all layers of the anterolateral abdominal wall are fused.
Recall that the linea alba is formed as a result of an “interweaving” of the aponeuroses of the external oblique, internal obligue and transversus abdominus mm.
Lateral to the rectus abdominis m.on each side, identify the linea semilunaris. These paired and slightly curved vertical lines represent the lateral border of the rectus sheaths which enclose the rectus abdominis muscle on each side.
Identify the inguinal ligament running between the ASIS and pubic tubercle. This ligament is the inferior thickened border of the aponeurosis of the external oblique muscle. The inguinal canal runs parallel to and superior to the medial half of the inguinal ligament.
The inguinal canal runs parallel to and superior to the medial half of the inguinal ligament. It extends from the superficial inguinal ring (an opening in the aponeurosis of the external oblique m.) and the deep (internal) inguinal ring. The superficial inguinal ring is the opening in the aponeurosis of the external oblique m. through which the spermatic cord of the male or the round ligament of the female passes to the scrotum or labia majora.
Open the anterior wall of the rectus sheath by making a vertical incision parallel and 2 – 3 cm lateral to the linea alba from the pubic symphysis to the xiphoid process.
From each end of the vertical incision, make a transverse incision towards linea semilunaris.
Reflect the anterior portion of the rectus sheath laterally.
Identify the tendinous intersections that divide the rectus abdominis m. into segments, and serve as attachment sites for the rectus abdominis m. to the overlying sheath.
You may see the thoracoabdominal nerves (ventral rami of T6 – T12) which innervate the rectus abdominis m. piercing the anterior layer of the sheath.
You should be able to identify the small pyramidalis m., which is described as being triangular in shape. (It is actually absent in approximately 20% of people.) It is responsible for ‘tensing’ the linea alba.
Use your fingers to free the medial edge of rectus abdominis muscle from the linea alba.
Make a horizontal incision through the entire width of the rectus abdominis muscle at the level of the umbilicus.
Reflect the segments of transected muscle superiorly and inferiorly.
You can now examine the posterior surface of the rectus sheath. Approximately midway between the umbilicus and the pubic symphysis, the posterior wall of the sheath becomes much thinner. Identify the slightly curved, inferior margin of the thickened portion of the rectus sheath which is called the arcuate line. Above the arcuate line, the posterior layer of the rectus sheath is formed by the posterior layer of the aponeurosis of the internal abdominal oblique muscle and the aponeurosis of the transversus abdominis muscle. Below the arcuate line the posterior layer of the rectus sheath is formed by the transversalis fascia
Make a longitudinal incision along the anterior axillary line through the external obligue m. from the costal margin to the iliac crest. From the inferior end of this incision, make a second incision passing inferiorly and anteriorly through the external oblique m. and its aponeurosis, ending at the upper border of the superficial inguinal ring.
Next, detach the external oblique m. from the ribs. Reflect the cut portion of the external oblique m..
Superior to the arcuate line, the aponeurosis of internal oblique m. splits and contributes to both the anterior and posterior layers of the rectus sheath. Inferior to the arcuate line, the entire aponeurosis of the internal oblique m. passes anterior to the rectus abdominis muscle.
With the external oblique m. reflected, identify again the iliohypogastric n..
Make a longitudinal incision in the internal oblique m. parallel to the incision made in the external oblique m.. Begin separating the internal oblique m. from the underlying transversus abdominis m.. This will probably be a bit more difficult than separating the external oblique m. from the internal oblique m.. Vessels and nerves are the key to identifying this plane.
Reflect the internal oblique m. toward the linea semilunaris.