Download
1 / 18
250 likes | 652 Views
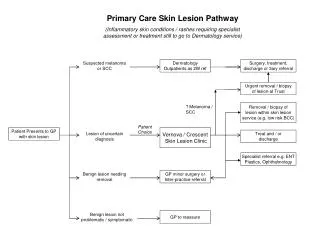
The Skin lesion. University of Florida Oral Exam Review. Introduction. Main goal is to differentiate benign vs. malignant lesions DDx benign: nevi, keratosis, hemangioma , granuloma, dermatofibroma , angiokeratoma DDx malignant: basal cell carcinoma, squamous cell carcinoma, melanoma.

E N D
The Skin lesion University of Florida Oral Exam Review
Introduction Main goal is to differentiate benign vs. malignant lesions DDx benign: nevi, keratosis, hemangioma, granuloma, dermatofibroma, angiokeratoma DDx malignant: basal cell carcinoma, squamous cell carcinoma, melanoma
BCC SCC
History • Assess melanoma risk factors • Family history – familial atypical mole, melanoma syndrome • Previous history of melanoma • Sunburn hx • History of the lesion • Change in size, shape, color, itching, bleeding • Signs of transformation • Race – white race 20x increased risk compared to black race
Physical examination • Multiple benign nevi higher risk of melanoma • ABCDE • Asymmetry • Irregular Borders • Variegated (mixed) Color • Large Diameter (>6mm) • Elevated surface • In-transit metastases • Palpate lymph nodes Skinipedia.org
Labs and Imaging • Skin biopsy • Not shave bx • Staging and metastases • Serum lactose dehydrogenase (LDH) level • Liver function tests (Liver #2 metastasis) • Chest X-ray (Lung #1 most common metastasis) • CT, MRI, PET-CT
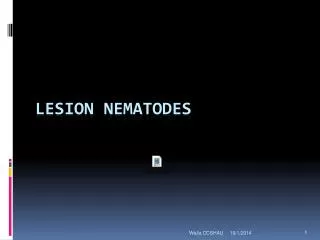
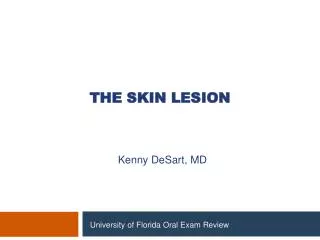
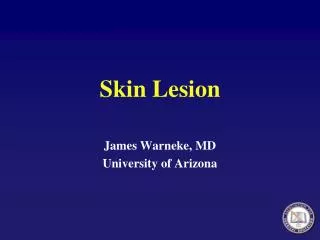
Types of Melanomas • Superficial spreading – most common (70%) • Arises from pre-existing nevi • Nodular – aggressive (15-30%) • Mostly vertical growth (no radial growth) • Can rarely lack pigment • High metastatic rate • Lentigomaligna – older patients (4-10%) • Typical over face, typically large (>3cm) • Arises from macular brown nevus • Less aggressive, best prognosis • Acrallentiginous – palms or soles in patients with dark skin (2-8%) • Most aggressive • Highest metastatic rate • Ocular melanoma – most common non-cutaneous melanoma
Superficial spreading Sabiston 18th edition
Nodular Sabiston 18th edition
Lentigomaligna Sabiston 18th edition
Acrallentiginous Sabiston 18th edition
Staging • Level of invasion (Clark staging) • Limited use, low predictive value • Depth of invasion (Breslow staging) • Used in American Joint Committee of Cancer (AJCC) TNM classification
TNM Classification • Tumor – a (no ulceration), b (ulceration) • T1 ≤ 1 mm • T2 1.01-2 mm • T3 2.01-4 mm • T4 >4 mm • Node • N1 – 1 node • N2 – 2-3 nodes • N3 – 4+ nodes • Metastasis • M1a – distant skin, subq, or lymph node and normal LDH (lactate dehydrogenase) • M1b – lung metastases with normal LDH • M1c – Visceral metastases with normal LDH • OR any distant metastases with elevated LDH
Surgical Treatment • Wide local excision (WLE) is the cornerstone of treatment • Margin of excision depends on depth • <1mm: 1cm margin • >1mm: 2cm margin • Primary closure or skin graft • Sentinel lymph node biopsy • Not needed if <1mm (WLE 95% cure • Unless Clark’s IV or V • Perform in >1mm and no clinically evident nodes
Surgical Treatment • Positive regional lymph nodes – consider radiation therapy • Ajuvant therapy – chemo/radio/immunotherapy Unboundmedicine.com
Melanoma Pearls • Prognosis • Tumor thickness is most important • Ulceration also important • Distant metastases • Lung > liver > brain > bone • Survival is 11mo for lung, 2-6 mo for others • Solitary brain metastasis should be resected • Can bleed, some can live 5+ years with resection and radiation therapy • The most common type of metastasis to small bowel is melanoma
Other Pearls SCC and BCC can generally be resected with 4-6mm margins SCC and BCC can be resected with MOHS