Download
1 / 22
220 likes | 454 Views
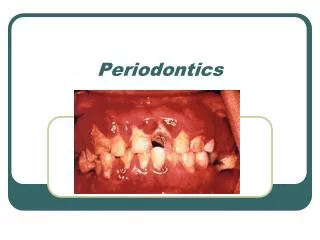
Pre-clinical Periodontics. Dr Jamal Naim PhD in Orthodontics. Periodontitis/ attachment loss. Furcation involvements. It refers to the invasion of the bifurcation or trifurcation of multirooted teeth by periodontal disease. The first lower molars are the most common site

E N D
Pre-clinical Periodontics Dr Jamal Naim PhD in Orthodontics Periodontitis/ attachment loss
Furcation involvements It refers to the invasion of the bifurcation or trifurcation of multirooted teeth by periodontal disease. • The first lower molars are the most common site • Maxillary premolar the least common • The number of involvements increases with age • Clinically it can be visible or covered by the wall of the pocket
Furcation involvements • The extent of involvement is determined by probing with a blunt probe • Involvement has been classified in 4 Grades according to tissue destruction
Furcation involvements • Grade I: incipient involvement • Grade II: partial bone loss (Cul De Sac) • Grade III: total bone loss with through-and through opening of the furcation • Grade IV: similar to III with gingival recession exposing the furcation.
Furcation involvements • No involvement, only intrabony pocket
Furcation involvements • Grade I: incipient involvement
Furcation involvements • Grade II: partial bone loss (Cul De Sac)
Furcation involvements • Grad III: total bone loss with through-and through opening of the furcation
Furcation involvements • Grade IV: similar to III with gingival recession exposing the furcation.
Furcation involvements • Furcation involvements can occur buccolingual and also mesiodistal (Upper molars)
Furcation involvements • The anatomy of the bifurcations in the mandible is less complicated than that of the maxillary teeth. • Almost of lower teeth roots exhibit some depressions, that makes plaque accumulation easier
Furcation involvements • The anatomy of the bifurcations in the mandible is less complicated than that of the maxillary teeth. • Almost of lower teeth roots exhibit some depressions, that makes plaque accumulation easier
Furcation involvements Mesial Furcation involvement of upper 2. molar
Furcation involvements Buccal Furcation involvement of upper 2. molar
Furcation involvements Distal Furcation involvement of upper 2. molar
Etiologic factors of furcation involvements • Trauma from occlusion • Enamel projections • Short root trunk • Accessory pulpal canals in the furcation area
Furcation involvements Long term follow-up of periodontal treatment indicates periodontal lesions in the majority of patients will respond well. The one exception to this seem to be lesions in multi-rooted teeth that have advanced into the furcation area between the roots. (Hirschfield 1978, McFall 1982, Goldman 1986)
Furcation involvements In teeth with furcation lesions a tooth mortality rate for periodontal reasons of 31% - 57% has been observed over periods averaging about 20 years compared to an overall tooth mortality for all teeth of only 7% - 10%. (Hirschfield 1978, McFall 1982)
Causes of Bone loss • Extension of gingival inflammation • Occlusal trauma • Systemic disorders • Local and anatomic factors
Occlusal trauma • Trauma from occlusion can produce bone destruction in the presence or absence of inflammation • In the absence of inflammation the bone changes caused by trauma vary from: • Increased compression and tension • Increased osteoclasis • Necrosis of PDL and bone • Resorption of tooth and bone
Occlusal trauma • These changes are reversible • Persistent trauma can modify the bone shape and increase tooth mobility • Combined with inflammation, trauma can aggravate the bone destruction
Systemic diseases • Local and systemic factors regulate the physiologic equilibrium of bone • Some systemic diseases cause a tendency toward bone resorption • In this cases the bone loss caused by periodontal diseases will be magnified • Osteoporosis results in loss of bone minerals and in structural changes • Hyperparathyroidism and langerhans cell histiocytosis are other examples