Download
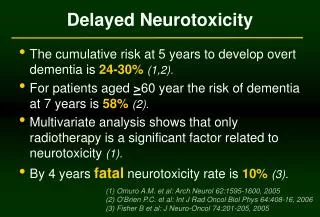
1 / 38
500 likes | 1.04k Views
Anaesthesia and Neurotoxicity. Andrew Davidson Royal Children’s Hospital Melbourne AUSTRALIA. http://www.smarttots.org. Rodent data up to 2010. Neuronal apoptosis in rodent models Ketamine, isoflurane, midazolam, propofol, sevoflurane Dose effect Combination worse

E N D
Anaesthesia and Neurotoxicity Andrew Davidson Royal Children’s Hospital Melbourne AUSTRALIA
Rodent data up to 2010 • Neuronal apoptosis in rodent models • Ketamine, isoflurane, midazolam, propofol, sevoflurane • Dose effect • Combination worse • Window of vulnerability day 7 in a rat • Some evidence for long term neurobehavioural effect
Mechanism • May be related to inactivity • May be related to changing ontogeny of receptors • May be due to upregulation of NMDR receptor
Slikker et al. Ketamine-Induced Neuronal Cell Death in the Perinatal Rhesus Monkey. Toxicological Sciences 2007; 98: 145-158 • Ketamine in monkeys • Apoptosis • 24 hours ketamine, 5 day old monkey • No apoptosis • 3 hours ketamine, 5 day old monkey • 24 hours ketamine, 35 day old monkey • Big doses • Need big doses in monkeys to have an effect
Day 6 monkeys • 5hrs isoflurane 0.7-1.5% • Increased apoptosis
Paule et al. Ketamine anesthesia during the first week of life can cause long-lasting cognitive deficits in rhesus monkeys. Neurotoxicol Teratol 2011 • Monkeys exposed to 24 hrs ketamine as day 5 infants • Now 3½ years old: cognitive impairments • poorer performance in learning and colour and position discrimination tasks • deficits in accuracy of task performance & response speed • differences in motivation
Ketamine Control Propofol Day 15 rat pups 5hrs anaesthesia: propofol, ketamine, midazolam Increased dendritic spine density
Control 60 min 120 min 30 min Day 16 rat pups Isoflurane, desflurane, sevoflurane 30, 60, 120 minutes No cell death Increased spine density
Which agents are bad? • Isoflurane, desflurane, sevoflurane
Which agents are bad? • Isoflurane, desflurane, sevoflurane • Midazolam, diazepam, clonazepam • Phenobarbital, pentobarbital • Chloral hydrate • Propofol
Which agents are good? • Dexmedetomidine, xenon • no apoptosis • “protective” • Opioids • no evidence for apoptosis
Problems with animal studies • Duration of exposure • Dose of agent • Monitoring • Length of neurodevelopment • Plasticity • Effect of surgery
Lumbar intrathecal morphine • Rats – P3, P10, P21 • Therapeutic dose • Toxicity • Therapeutic index
Therapeutic index • Toxic dose/effective dose • P3: >3/0.01 >300 • P21: >3/0.15 >20
Rats; P3, P7, P21 Ketamine; 3-10 mg/kg Effective dose Toxicity Therapeutic index
Therapeutic index Toxic dose/effective dose P3 3/3 1 P21 15/15 1
2008 Mayo Clinic study • 5357 children in a population based retrospective birth cohort • “Rochester epidemiology project” • Register of all children born 1976-82 in five townships in Olmsted county Minnesota who stayed local for 5 years • 593 surgery before age of 4 • Adjusted for gender, birth weight, gestational age • 932 had learning disability
Dose effect – increased risk of disability with duration and number of anaesthetics
J Neurosurg Anesth • 383 children born in NY state cared for by Medicaid that had a hernia repair < 3yrs of age • 5050 randomly selected controls matched on age • Adjusted for age, gender, race and presence of complicating diagnoses at birth • Behavioral or developmental disorder • 17 in hernia group (4.4%) • 59 in non-hernia group (1.2%) • Adjusted Hazard Ratio 2.3 (1.3 - 4.1)
Danish birth cohort 1986-1990 2689 inguinal hernia repair 14,575 Controls (5% of all children in Denmark) Outcome school test at 9th grade (age 15-16 years) Hernia group do worse No evidence for an association when adjusted for confounding factors
Twin study: monozygotic concordant-discordant design 1143 monozygotic twin pairs born 1986-95 Any anaesthesia Prior to 3 Prior to 12 Educational achievement at age 12 Twin Research and Human Genetics 2009
Problems with human studies • Little idea which age is most at risk & many studies have older children • No idea how long an exposure is bad • Bias is difficult to eradicate in cohort studies that compare to population norms • Little idea which outcome to look at & many studies have multiple outcomes and very course outcomes • Confounding • Many known strong confounding factors • Probably many unknown confounding factors • Adjustments are not perfect & BIG doesn’t really help
Anaesthesia is associated with surgery Surgery is associated with pathology
Hormonal “Stress” Inflammatory response Circulatory instability Respiratory compromise Extra lines & handling Temperature instability Surgery poor outcome
Genetic abnormality Malformations Prematurity Sepsis Pathology poor outcome
Surgery or anaesthesia? • Not able to disentangle effect of surgery and anaesthesia • Surgery may be the harm • Anaesthesia may have benefits to reduce surgical harm
Anaesthesia Bad Good Reduces stress Reduces pain Neuro protection Apoptosis Dendritic development Effects may be disproportionate in different situations
Summary Animal evidence Strong for histological change Some evidence for change in function Human evidence Some evidence for an association between surgery/anaesthesia and poor outcome Role of anaesthesia very unclear
Recommendations • “Avoid elective surgery in infants” • Don’t withhold analgesia and anaesthesia for necessary surgery and procedures • Is one drug better ? • Avoid prolonged use of high dose ketamine in infants • Dexmedetomidine, opioids may be preferable • Be very careful changing safe established practices due to theoretical risks
Future studies • GAS study • RCT hernia GA versus RA • Raine cohort • Western Australian birth cohort • PANDA study • Hernia repair and matched