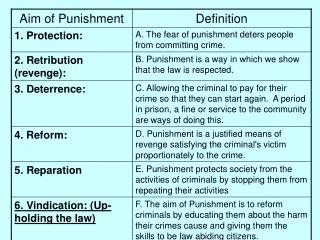
Download
1 / 18
180 likes | 270 Views
The Gemini Study Saquinavir/r (SQV/r) vs lopinavir/r (LPV/r) plus emtricitabine/tenofovir (FTC/TDF) as initial therapy in HIV-1 infected patients. Walmsley S, 1 Ruxrungtham K, 2 Slim J, 3 Ward D, 4 Larson P, 5 and Raffi F 6.

E N D
The Gemini StudySaquinavir/r (SQV/r) vs lopinavir/r (LPV/r) plus emtricitabine/tenofovir (FTC/TDF) as initial therapy in HIV-1 infected patients Walmsley S,1 Ruxrungtham K,2 Slim J,3 Ward D,4Larson P,5 and Raffi F6 1University of Toronto, Toronto, Canada; 2HIV-NAT, Thai Red Cross AIDS Research Centre, Bangkok, Thailand; 3St Michael’s Medical Center, Newark, NJ, USA; 4Dupont Circle Physicians Group, Washington DC, USA; 5 Roche, Nutley, NJ, USA;6University Hospital, Nantes, France.
Gemini: Study Design • Prospective, randomized, multicenter, open-label trial • N = 337 • USA, Canada, France, and Thailand • Duration = 48 weeks • Inclusion criteria • Treatment naive • CD4 count ≤350 cells/mm3 • HIV-1 RNA >10,000 copies/mL • Exclusion criteria • Previous treatment with antiretrovirals (≥2 weeks exposure) • Evidence of OI or intercurrent illness 1:1 randomization Saquinavir/Ritonavir (SQV/r) 1000 mg/100 mg BID + FTC/TDF 200 mg/300 mg QD Lopinavir/Ritonavir (LPV/r) 400 mg/100 mg BID + FTC/TDF 200 mg/300 mg QD
Gemini: Subject Disposition 337 participants 170 participants randomized to LPV/r (ITT) 167 participants randomized to SQV/r (ITT) 163 in safety analysis 168 in safety analysis 148 in per-protocol analysis (PP)* 145 in per-protocol analysis (PP)* 128 participants reached week 48 135 participants reached week 48 *17 participants in SQV/r and 25 in LPV/r arm excluded from PP analysis primarily because of entry criteria violations: HIV-1 ≤10,000 copies/mL, CD4 count >350 cells/mm3, and HBsAg+.Two additional participants in the SQV/r arm were excluded: 1 for use of prohibited medication and 1 for a major protocol violation.
Gemini: Study Objective and End Points To demonstrate non-inferiority SQV/r vs LPV/r at week 48 in treatment-naïve, HIV-1 infected adults • Non-inferiority defined as lower CI threshold of −12% • Primary efficacy end point • Patients (%) with HIV-1 RNA <50 copies/mL at week 48 • Secondary efficacy and tolerability endpoints • Time course of virologic suppression (<50 copies/mL and <400 copies/mL) • Time course of CD4 cells/mm3 increase • Safety as assessed by clinical and laboratory AEs, SAEs, and deaths
Gemini: Demographics and Baseline Characteristics* *ITT Population; lipid data-safety population
Gemini: Subject Discontinuations a7 total: 3 deaths occurred outside of treatment period in LPV/r group (after withdrawal or during follow-up period): hepatic failure (possibly related to study drug), Burkitt's lymphoma, PML bCause of death: victim of crime (remotely related to study drug), drowning, sepsis cCause of death: suicide
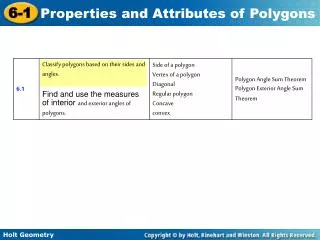
100 LPV/r <50 copies/mL (n = 170) SQV/r <50 copies/mL (n = 167) 80 64.7% 60 % Patients (95% CI) 63.5% 40 20 0 0 4 8 12 16 20 24 28 32 36 40 44 48 Week *ITT population: subjects randomized and received at least 1 dose of trial medication Gemini: HIV-1 Virological Response (ITT*; missing = non-response)
100 LPV/r <50 copies/mL (n = 170) SQV/r <50 copies/mL (n = 167) 80 64.7% 60 63.5% 40 SQV/r is non-inferior to LPV/r Estimated difference in response week 48 vs LPV/r for non-inferiority: PP = 3.5% (96% CI –8.1–15.0) p < 0.0058 Estimated difference in response week 48 vs LPV/r for non-inferiority: ITT = 1.14% (96% CI –9.6–11.9) p < 0.0119 20 0 0 4 8 12 16 20 24 28 32 36 40 44 48 Week *ITT population: subjects randomized and received at least 1 dose of trial medication Gemini: HIV-1 Virological Response (ITT*; missing = non-response) % Patients (95% CI)
167 146 157 154 149 145 142 142 133 126 SQV/r n = 153 170 160 150 146 147 141 140 140 133 LPV/r n = Week 0 4 8 12 16 20 24 28 32 36 40 44 48 -0.5 LPV/r p = 0.62 SQV/r -1.5 HIV-1 RNA (Log10 Copies/mL [±SD]) -2.5 -3.36 -3.5 -3.39 -4.5 *ITT population: subjects randomized and received at least 1 dose of trial medication Gemini: HIV-1 Viral Load, Mean Change From BL (ITT*; observed values)
250 204 LPV/r SQV/r 200 178 150 p = 0.33 100 50 0 0 4 8 12 16 20 24 28 32 36 40 44 48 Week SQV/r n = 153 137 166 138 141 121 142 129 148 143 *ITT population: subjects randomized and received at least 1 dose of trial medication LPV/r n = 152 169 142 130 133 139 138 140 141 148 Gemini: Absolute CD4 Median Change From BL (ITT*; observed values) CD4 Cells/mm3(95% CI)
Gemini: Adverse Events (all grades) *Multiple occurrences of the same AE in one individual are counted only once
Gemini: Virological Failures* *Virological failure defined as 2 consecutive counts of HIV RNA >400 copies/mL at week 16 or after aDocumented poor adherence; also had M184V bNew PI mutations were described at week 24 in 2 separate subjects. On further ongoing analyses, in 1 subject, the D60E mutation was subsequently confirmed in the baseline sample; for the subject presented here, L10I/V was confirmed to be new, but baseline sample could not be amplified past codon 46
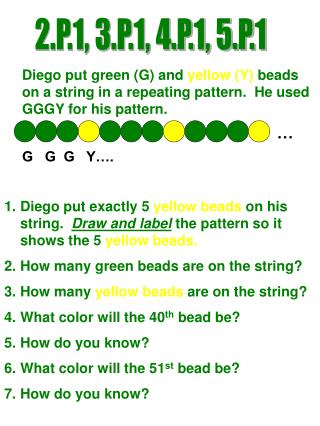
SQV/r LPV/r TC LDL HDL TG 100 p = 0.0007 p = 0.0022 55 80 p = 0.1300 p = 0.3912 45 60 Median Change mg/dL (95% CI) p = 0.4436 p = 0.3615 31 40 p = 0.4534 p = 0.9954 26 19 25 14 18 16 10 11 20 6 9 11 9 8 0 n = 106 109 81 100 105 108 80 99 105 108 80 99 106 108 81 99 Week 24 48 24 48 24 48 48 24 Baseline levels, median (mg/dL) SQV/r LPV/r 157.0, n = 130 152.0, n = 134 89.0, n = 129 89.0, n = 133 35.0, n = 129 38.0, n = 133 117.0, n = 130 117.0, n = 133 Gemini: Median Change in Fasting Lipid Levels (mg/dL)
Week 24 Week 48 SQV/r LPV/r n = 105 108 80 99 -0.1 TC/HDL -0.13 -0.07 -0.3 -0.5 -0.27 -0.40 Baseline ratio SQV/r LPV/r 4.25, n = 129 4.29, n = 133 p = 0.4727 p = 0.0237 Gemini: Median Change in Fasting TC/HDL Ratio
60 SQV/r LPV/r 50 39 40 34 33 31 % Patients 30 24 24 23 19 20 14 13 11 11 10 9 10 2 2 2 1 0 n= 130 134 127 125 96 116 129 133 127 125 96 116 130 133 127 125 96 116 BL BL Wk 24 Wk 24 Wk 48 Wk 48 BL Wk 24 Wk 48 TG ≥400 mg/dL LDL ≥130 mg/dL TC ≥200 mg/dL Gemini: Subjects Exceeding Lipid Levels that May Warrant Clinical Intervention* *Based on NCEP and ACTG guidelines; fasting samples
Gemini: Conclusions • Gemini demonstrates non-inferiority of SQV/r (% subjects reaching VR <50 copies/mL) to LPV/r in the treatment of HIV-1 infected ARV-naïve adults • In this study population with advanced untreated HIV disease, both regimens showed substantial CD4 cell count increases • Adverse events were reported with similar frequency and resulted in few discontinuations in either arm • Significantly lower elevations from baseline in median triglycerides were observed with SQV/r at weeks 24 and 48 • Decrease in TC/HDL ratio for SQV/r at week 24 (but not at week 48) was significantly greater than for LPV/r
Gemini: Conclusions • Overall, these results confirm that SQV/r is an efficacious and well-tolerated PI for use in treatment-naïve patients with HIV-1 infection • Gemini provides further evidence for the lack of emergence of PI resistance with failure of first-line boosted PI regimens
The following investigators: Jonathan B. Angel, MD Christian Aquilina, MD Jean-François Bergmann, MD, PhD Robert Bolan, MD Philip Brachman, MD U. Fritz Bredeek, MD, PhD Jason Brunetta, MD Robert Catalla, MD Catherine Creticos, MD Charles P. Craig, MD Frederick A. Cruickshank, MD Yasmine Debab, MD Edwin DeJesus, MD Pierre Dellamonica, MD Serge Dufresne, MD Joseph Gathe, Jr, MD Barbara Hanna, MD Dushyantha Jayaweera, MD Joseph G. Jemsek, MD Harold Katner, MD Richard Lalonde, MD Jean-Marie Lang, MD, PhD Gilead Sciences Inc for provision of Truvada® Caroline Lascoux-Combe Jean-Michel Livrozet, MD Mona Loutfy, MD, MPH Iván Meléndez-Rivera, MD Karam Mounzer, MD Gerald Pierone, MD Isabelle Poizot-Martin, MD, PhD David Prelutsky, MD Anita R. Rachlis, MD, MEd François Raffi, MD Isabelle Ravaux, MD Kiat Ruxrungtham, MD Dominique Salmon, MD, PhD Anne Simon, MD Jihad Slim, MD Fiona M. Smaill, MD Christian Trepo, MD, PhD Benoit Trottier, MD Sharon Walmsley, MSc, MD Douglas J. Ward, MD Yazdan Yazdanpanah, MD, MSc David Zucman, MD Gemini: Acknowledgements Subjects who participated in this study



![A = p 4 B = p 5 CP = E[ p 7 , p 2 , p 3 , p 6 , p 1 , p 8 ] S[p 4 , p 5 ] d min = d 45](https://cdn3.slideserve.com/6420476/slide1-dt.jpg)