Download
1 / 90
960 likes | 1.28k Views
Post-mortem Toxicology. Dr A J Jeffery MBChB MD FRCPath (Forensic) MFFLM Home Office registered forensic pathologist. Areas to Cover. Why take toxicology What samples How to take them What does the toxicologist do with the samples? How to interpret the results – general considerations

E N D
Post-mortem Toxicology Dr A J Jeffery MBChB MD FRCPath (Forensic) MFFLM Home Office registered forensic pathologist
Areas to Cover • Why take toxicology • What samples • How to take them • What does the toxicologist do with the samples? • How to interpret the results – general considerations • Alcohol • Drugs of abuse • Toxicology in other causes of death • Other specimens • Case examples
WHY TAKE TOXICOLOGY ?
Why take toxicology ? • To ascertain if the deceased was under the influence of alcohol or drugs of abuse at the time of their death. • RTAs / Accidental deaths / suicides • To confirm or refute overdose / poisoning • To confirm presence / levels of therapeutic drugs. • Eg epilepsy / antidepressants
WHAT SAMPLES ARE APPROPRIATE ?
Samples • Blood (plain) (peripheral) • Blood (preserved) (peripheral) • Urine (plain) • Urine (preserved) • Fluoride – inhibits further alcohol production but won’t undo the damage already done. • Vitreous • Stomach Contents • Tissues • Liver (mid R lobe) • Skeletal muscle (eg psoas) (if embalmed buttock)
OBTAINING THE BLOOD SAMPLE
Femoral Vein Sampling • Vein NOT artery • Before evisceration • Before urine sampling • Ideal = tie off / clamp, then sample by wide-bore needle below • Routine = clean catch • Ideal = don’t milk the leg • Routine = required to gain sufficient sample
Problem: MINIMAL FEMORAL BLOOD
Insufficient Femoral Blood • Take what ever you can in preserved tubes • Subclavian = reasonable alternative • Could take free-lying chest blood etc for screening for the general presence of drugs • Make sure you say where each sample has come from • Obtain an alternative specimen
OBTAINING THE URINE SAMPLE
Urine Sampling • Needle and syringe or • Open dome of bladder and aspirate with syringe alone • Presence of a catheter may be important toxicologically as the urine may contain artefactually high lignocaine due to catheter lubricant gel
WHAT DO THE TOXICOLOGISTS DO WITH THE SAMPLE ?
Analysis • Screening (GC / Immunoassay) • What classes of drug are present • Confirmation (GCMS) • Specific drugs found by breaking them down & looking at the breakdown products. • Quantification • Technique may vary dependent on the nature of the drug being analysed.
HOW TO INTERPRET THE RESULTS
General Considerations • Accuracy of reference ranges • Re-distribution – site matters! • Individual variation (e.g. renal disease) • Decomposition • Tolerance
Accuracy of reference ranges • Interpretation of absolute drug levels / Reference ranges • Based on individual reports • Variable from lab to lab due to varying techniques • Need to consider the previous list
General Considerations • Re-distribution – site matters! • Individual variation (renal disease) • Decomposition • Tolerance
Redistribution • Discovered with digoxin • Most drugs that undergo redistribution do so because of their relative lipid solubility. • Due to • Loss of cell integrity • Diffusion • GI tract – to adjacent structures • Through conduits – lymph • Diffusion from bladder
Natural Disease • Depends or route of administration • 1st pass / second pass metabolism • Absorption • With or without meal • GI surgery • Elimination / Clearance • Renal impairment • Liver impairment
Decomposition • Significant redistribution • Some drug levels increase • Alcohol production by bacterial action • Others degrade • If there is a degree of decomposition make sure you write it on the tox request
Tolerance • Increasing doses required over time to achieve same effects. • What is lethal to a naïve user may have no effect at all in a chronic user. • First dose deaths • People walking around and working with enough drugs on board to kill an elephant! • Prison release deaths
Deaths due to Alcohol • What alcohol related causes of death do you know? • How might you classify them? • Which specific toxicological causes do you know?
Alcohol • Acute alcohol toxicity • Ketoacidosis • Alcohol in combination with other drugs
Problems with Interpretation of Alcohol • Redistribution • Dealing with decomposition • Back calculations
Acute alcohol toxicity • How does it cause death? • Death – respiratory depression due to action on brainstem • UK legal driving limit? • Driving limit 80 mg/100ml • Less than 20 mg/100ml generally considered insignificant. • >30 = higher skills • 30 – 50 = deterioration in driving • 50 – 100 = inhibitions / laughter • 100 – 150 = slurring, insteadiness, poss nausea • 150 – 200 = obvious drunkenness, nausea staggering • 200 – 300 = stupor, vomiting, coma • 300 + = stupor, coma, aspiration &
Alcohol – fatal level or not? • LD 50 = 400 mg/100ml • Alcohol has symbiotic relationship with other drugs. e.g. • < 200mg/100ml can be fatal if opioids are taken. • > 200mg/100ml can ½ the fatal dose of opioids • > 100mg/100ml may enhance heroin toxicity • Ethyl glucuronide (minor breakdown product) in urine if imbibed within 5 days of death.
What is ketoacidosis? • Can you explain why this happens?
Ketoacidosis • Brain can utilise ketone bodies when glucose is unavailable – fasting / starvation • Ketone bodies, formed by the breakdown of fatty acids and the de-amination of amino acids. • Ketoacidosis is an extreme and uncontrolled form of ketosis, which is a normal response to prolonged fasting. In ketoacidosis, the body fails to adequately regulate ketone production causing such a severe accumulation of keto acids that the pH of the blood is substantially decreased. • Alcoholic ketoacidosis • Metabolic acidosis • Malnutrition • Binge drinking superimposed on chronic alcohol abuse
Ketoacidosis • Ketones: • Acetone (can be produced pm) • <0.5 mg/100ml • Beta hydroxybutyrate (less likely to be raised artefactually) • <0.5 mmol/L • 1.26 – 47.2 mmol/L (assoc with fatalities) • Causes • Alcoholic ketoacidosis • Diabetic ketoacidosis
Alcoholic vs Diabetic • How might you differentiate? • Urine glucose • HbA1c • 4 - 6.1%
Calculations • AVOID ! • Clearance • 10 – 25 mg/dl/hr ( about a unit an hour) • In 10 hours you can clear ~ 100-200 mg/dl • Alcoholics can clear 30 – 40 mg/dl/hr (due to training!) • Widmark equation • Used by some to predict amount of alcohol consumed
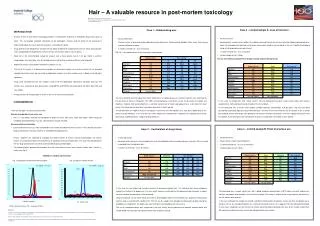
Decomposition • 70 – 190 mg/100ml reported as artefact • Consider pm findings • Look for other substances produced pm • Use vitreous and urine as supportive evidence • These are relatively protected from redistribution • Normal ratios (if in equilibrium) • Urine : Blood Vitreous : Blood 1.23 : 1 1 : 0.81
Drugs of Abuse OPIOID AGONISTS SYMPATHOMIMETICS
Opioid agonists • Analgesia / euphoria / dysphoria • Respiratory depression • miosis
Morphine and other opioids • Morphine • Heroin (diamorphine) – IV, smoked, sniffed • Methadone (green liquid – oral or IV) • Pethidine, buprenorphine • ** CNS depression **
Findings • History / scene / paraphernalia • External • iv sites • Foam at nose / mouth • Limited & non specific • Pulmonary congestion and oedema • Stomach contents – methadone is usu green!
Morphine / Heroin • Heroin / diamorphine – synthetic morphine derivative • Powerful opioid analgesic • Metabolised almost immediately (10 – 15 mins) to 6 monoacetyl morphine 6MAM and then within 24 hours to morphine. • Presence of 6MAM is consistent with use within 12-24 hours • Ie recent intake / top up injections • Acute alcohol intoxication potentiates the effects
Total morphine : Free Morphine • Gives some idea of time since administration • Eg in IV admin • 15 mins post admin 4 : 1 • 60 mins 9 : 1 Therapeutic Lethal_______ • Free morphine 10 – 100ng/ml 50 – 4000 ng/ml
Heroin • A contaminate of street heroin is acetylcodeine • Hence may have +ve codeine levels • Most heroin deaths occur several hours after taking the drug • Sleepy / snoring • May have time to metabolise drug despite irreversible respiratory depression
Methadone • Therapeutic • 75 – 1100 ng/ml • Toxic • 200 – 2000 ng/ml • Lethal • 400 – 2000 ng/ml • Significant overlap • Tolerance becomes very important • Interpretation requires knowledge of drug history • Long & variable T ½
Methadone • Breakdown product – EDDP • This is inactive • Titration is important • Many deaths occur during first few weeks of treatment • Can cause respiratory depression at therapeutic doses • Lipophilic so undergoes significant redistribution • Even peripheral samples can be 2x in and 3x in
Opioids • Tolerance = V V important consideration • Eg. Prison release • Palliative care • Nb worth remembering that 10% of codeine will breakdown to become morphine. Therapeutic Lethal_______ • Free Codeine 30 – 340ng/ml >1600 ng/ml
Sympathomimetics • Incr activity of adrenaline and serotonin • Adrenalin • Hypertension • Tachycardia • Mydriasis • Serotonin • Excitement • Hyperthermia
Stimulants • Cocaine • Amphetamine • Ecstasy • Other methamphetamines • Associated with subarchnoid haemorrhage • 80% of these assoc with aneurysms • Intracerebral haemorrhage • Associated with AVMs & hypertension
Findings • Hearts of stimulant users tend to be heavier than controls • Fibrosis • Contraction band necrosis • Accelerated atherosclerosis • Non specific pulmonary changes • Crack cocaine smokers – prominent anthracosis esp in alveolar macrophages & emphysematous changes.

![[Project Name] Post-Mortem](https://cdn0.slideserve.com/1273592/project-name-post-mortem-dt.jpg)