Download

1 / 35
370 likes | 724 Views
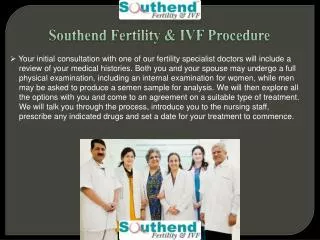
Reendodontic treatment ( possibilities apexlocators in endodontic therapy). Retreatment in endodontics. 21ST-CENTURY ENDODONTICS Endodontics as a discipline has offered patients the opportunity to maintain their natural teeth. As the population expands and ages,

E N D
Reendodontic treatment(possibilities apexlocators in endodontic therapy)
Retreatment in endodontics 21ST-CENTURY ENDODONTICS Endodontics as a discipline has offered patients the opportunity to maintain their natural teeth. As the population expands and ages, the demand for endodontic therapy can be expected to increase as patients seek dental options to keep their teeth for a lifetime.
Retreatment in endodontics • Over thepastdecade, nickeltitaniumrotaryinstrumentation, microscopicendodontics, digitalradiography, a plethoraofobturationsystems, and biocompatiblesealingmaterialshavehelpedpractitionersperformendodonticprocedures more effectively and efficientlythaneverbefore. • Diagnosis, in fact, has become more challenging. Overall, casemanagementis more complexasgeriatricpatients and thosewho are medicallycompromisedare more inclined to seektreatmenttosavetheirteeth.
Retreatment in endodontics • Endodontics has gonethroughmanychanges in thepastseveralyears. Bacterialculturingofcanals, theuseofsilverpoints, multipleendodonticvisits, radiographic “guessing” ofworkinglengths, and dependence on canalmedicaments are fadingconcepts in endodontictreatment. • Thanks to moderntechniquesused in endodontics, most oftheteeth, which in thepastwouldberemovedcurrentlycanbesaved. Manypatientshave had badexperiencesassociatedwiththe "rootcanaltherapy" and in thiscontextoften face a dilemma: whether to remove or cure? Thelatterapproachisirreversible and shouldbetreatedas a lastresort. We tried to makethetreatmentaslightaspossible, short and comfortable.
Retreatment in endodontics • A variety ofadvancements in technology,materials, equipment, and evenphilosophyhavechangedhowendodonticcases are managed. • Electronicapexlocatorsand surgicalmicroscopeshaveheightenedprecisionandeliminatedmuchoftheuncertaintyassociatedwithendodonticprocedures. Digitalradiography has expandeddiagnosticabilities and increasedtheability to communicatewithpatients and otherdentists.
Endodontic treatment consists of • removing the contents of the chamber and canal system-the pulp (a network of blood vessels and nerves) • the elimination of bacteria • filling tightly root canals
For that we use: • modern tools to process canals • systems for their filling • apex locator to measure the length of the root • dental RTG • endodontics microscope
EndodonticServices • RootCanalTherapy • WithRotarySystem • WithApexFinder • Re-EndodonticTreatment • Apicectomy • Hemisection • Re-ImplantEndodontic
Electronic apex locators • Prior to root canal treatment at least one undistorted • radiograph is required to assess canal morphology. • The apical extent of instrumentation and the final root • filling have a role in treatment success, and are primarily determined radiographically. • Electronic apex locators reduce the number of radiographs required and assist where radiographic methods create difficulty. • They may also indicate cases where the apical • foramen is some distance from the radiographic apex.
Theremovalofallpulptissue, necroticmaterial and microorganismsfromtherootcanalisessentialforendodonticsuccess. Thiscanonlybeachievedifthelengthofthetooth and therootcanalisdeterminedwithaccuracy. Theoutcomeoftreatmentofrootswithnecroticpulps and periapicallesionsisinfluencedsignificantly by theapicalleveloftherootfilling • Traditionally, the point ofterminationforendodonticinstrumentation and obturation has beendetermined by takingradiographs. Thedevelopmentoftheelectronicapexlocatorhas helpedmaketheassessmentofworkinglength more accurate and predictable .
The importance of working length • Grove (1930) statedthat ‘theproper point to which rootcanalsshouldbefilledisthejunctionofthedentin and thecementumandthatthepulpshouldbesevered atthe point ofitsunionwiththeperiodontalmembrane’. Thecementodentinaljunction (CDJ) istheanatomical and histologicallandmarkwheretheperiodontalligament begins and thepulpends. Rootcanalpreparation techniquesaim to makeuseofthispotentialnaturalbarrier betweenthecontentsofthecanal and theapicaltissues.
The importance of working length • Itisgenerallyacceptedthatthepreparation and obturationoftherootcanalshouldbeat or shortoftheapicalconstriction. An in vivohistological study foundthatthe most favourablehistologicalconditionswerewhentheinstrumentation and obturationremainedshortoftheapicalconstrictionandthatextrudedgutta-perchaandsealeralwayscaused a severe inflammatoryreactiondespitetheabsenceofpain . • Theproblemclinicians face ishow to accuratelyidentify and prepare to thislandmark – the‘workinglength’ – and achieve maximum success. Epidemiologicalstudieshavereportedthatthebestprognosisiswhentherootfilling lies within 2 mm oftheradiographicapex(Sjo¨grenet al. 1990). Thevariations in anatomyoftoothapicesboth by age and tooth type makethistaskallthe more challenging.
Anatomy of the apical foramen • To appreciate fully the concept of working length, an understanding of apical anatomy is required. The anatomy of the apical foramen changes with age. • Figure 1a shows a concept of the apex (a), the apex of a younger person (b) and the changing apex due to hard tissue deposition (c). (a) Position of the apical foramen (adapted from Kuttler 1955). (b) Anatomy of the root apex,
Anatomy of the apical foramen • Itisgenerallyagreedthatthere are threedistinctaspectsoftheapexthatmustbeappreciated. Figure 1b showstheseasthetoothapex (1), theapicalforamen [major foramen (2)] and theapicalconstriction [minorforamen (3)] whichisalsodescribedastheCDJ. • Theapicalforamenisnotalwayslocatedattheanatomicalapexofthetooth. Theforamenofthemainrootcanalmaybelocated to onesideoftheanatomicalapex, sometimesatdistancesofup to 3 mm in50–98% ofrootsDummeret al. (1984) reportedthemeanapex to foramendistance (Fig. 1b, 4) in anteriorteeth to be 0.36 mm. Thegeneral trend isthattheapex to foramendistanceisgreater in posteriorteeth and olderteeththan in anterior and youngerteeth.
Anatomy of the apical foramen • Theforamen to apicalconstriction (Fig 1(b)5) isapproximately 0.5 mm in theyoungergroup and 0.8 mm in theoldergroupforalltoothtypes • Traditionalmethodsforestablishingworkinglengthhavebeen(a)theuseofanatomicalaverages and knowledgeofanatomy, (b) tactilesensation, (c)moisture on a paper point and (d)radiography • .Radiographicdeterminationofworkinglength has beenusedformanyyears. Theradiographicapexisdefinedastheanatomical end oftherootasseen on theradiograph, whiletheapicalforamenistheregionwherethecanalleavestherootsurfacenext to theperiodontalligament (AmericanAssociationofEndodontists 1984).
Anatomy of the apical foramen • Whentheapicalforamenexits to thesideoftheroot or in a buccal or lingualdirectionitbecomesdifficult to view on theradiograph. • Thepreoperativeradiographisessential in endodontics to determinetheanatomyoftherootcanalsystem, thenumber and curvatureofroots, thepresence or absenceofdisease, and to actasaninitialguideforworkinglength. Theelectronicapexlocatorisaninstrument, whichusedwithappropriateradiographs, allowsformuchgreateraccuracyofworkinglengthcontrol
Apexlocators • Anelectronicmethodforrootlengthdeterminationwasfirstinvestigated by Custer (1918). • Thirdgenerationapexlocatorsare similar to the secondgenerationexceptthattheyusemultiplefrequencies to determinethedistancefromthe end ofthecanal. Theseunitshave more powerfulmicroprocessors and are able to processthemathematicalquotient and algorithmcalculationsrequired to giveaccuratereadings. • Therelativevaluesoffrequencyresponsemethoddetectstheapicalconstriction by calculatingthedifferencebetweentwodirectpotentialspickedupbyfilterswhen a 1 kHz rectilinearwaveisapplied to thecanal.
Apexlocators • Manyoftheproblemswithpreviousgenerationsofapexlocatorsoccurredwhentherootcanalcontainedmoisture-richsubstancessuchasexudate, electrolyteslikesodiumhypochlorite and theproductsofhemorrhage. The new third-generationapexlocatorshaveovercome most oftheseproblems, are more user-friendly and requireminimalcalibration. • More importantlyistherevelationthatmodern-dayapexlocatorsmayevenbemorereliablethanradiographicinterpretation. Studiesevaluatingapexlocatorshavedemonstratedaccuraciesofworkinglengthdetermination to within 0.5 mm fromtheapicalconstriction, rangingfrom 75 percent to 93.4 percent. Nonetheless, usingtoday’sapexlocatorin conjunctionwith a radiographisstillanextremelyeffectiveadjunctfordeterminingworkinglength and detectingperforations or rootfractures.
Apexlocators • Currentapexlocatorsutilizeanalternatingcurrentwithinthecanal and monitor theimpedancebetweenperiapicaltissue and oral mucosavia a lipclip. Thecircuitrywithinthemachinecalculatestheimpedancebetweenthefile tip and lipmucosa; theapexisdetectedusingthecalculatedimpedancevianeedlepointers, sounds, lights, digitalreads or variouscombinationsthereofdepending on themachineused.
Apexlocators • New technology in thisarea has resulted in microprocessorsthatmeasurefrequencyshifts and apicalcapacitances. • As a result, accuracyoftheselocators has improved, especially in thepresenceofanatomicalaberrations and canalmoisture. • ExamplesoftheseincludetheRoot ZX (J. Morita USA), theJustwo (MedidentaInternational) and theEndex (Osada Inc.). Someoftheseuseanalternatingcurrentofatleasttwofrequencies, and measureandcomparethetwoelectricalimpedances.
Apexlocators • Thismillenniumiscertain to delivereven more accurateapexlocators, perhapseventotallyeliminatingworkinglengthimages. • However, evenifthatgoalis never attained, there are obviousadvantageswiththethird-generationapexlocatorsavailabletoday. Theseincludeanaccurateworkinglengthdetermination, therebyreducingoverallradiationexposure, asonly a minimalnumberofimageswouldberequired. Withaccuratereadings, theremaybelesschancefor over- or underinstrumentation. Also, patienttreatmenttimewouldbereducedastheresultofthespeedatwhich a lengthcanbedetermined or verified.
Root Canals not suitable for Electronic Measurement Reading (EMR) Root Canal with a large apical foramen Root canal that has an exceptionally large apical foramen due to a lesion or incomplete development cannot be accurately measured; the results will show shorter measurement than the actual length. Root Canal with blood, saliva or a chemical solution overflowing from the opening If blood, saliva, or a chemical solution overflow from the opening of the root canal and contacts the gums, this will result in electrical leakage and an accurate measurement cannot be obtained. Wait for bleeding to stop completely. Clean the inside and opening of the canal thoroughly to get rid of all blood, saliva and chemical solutions and then make a measurement.
Broken crown If the crown is broken and a section of the gingival tissue intrudes into the cavity surrounding the canal opening, contact between the gingival tissue and the file will result in electrical leakage and an accurate measurement cannot be obtained. In this case, build up the tooth with a suitable material to insulate the gingival tissue. Fractured tooth Leakage through a branch canal Fractured tooth will cause electrical leakage and an accurate measurement cannot be obtained. A branch canal will also cause electrical leakage.
Re-treatment of a root filled with gutta-percha The gutta percha must be completely removed to eliminate its insulating effect. After removing the gutta percha, pass a small file all the way through the apical foramen and then put a little saline in the canal but do not let it overflow the canal opening. Crown or metal prosthesis touching gingival tissue Accurate measurement cannot be obtained if the file touches a metal prosthesis that is touching gingival tissue. In this case, widen the opening at the top of the crown so that the file will not touch the metal prosthesis before taking a measurement.
Cutting debris on tooth Pulp inside canal Thoroughly remove all cutting debris on the tooth. Thoroughly remove all the pulp inside the canal; otherwise an accurate measurement cannot be made. Caries touching the gums In this case, electrical leakage through the caries infected area to the gums will made it impossible to make an accurate measurement.
Blocked Canal The meter will not move if the canal is blocked. Open the canal all the way to the apical constriction to measure it. Extremely dry canal If the canal is extremely dry, the meter may not move until it is quite close to the apex. In this case, try moistening the canal with oxydol or saline.
Retreatment in endodontics • Retreatment in endodonticsprovides a secondchanceforthepatient to savethetooththatwouldotherwisebedeemedforextraction. • Treatmentapproachcanbeeithersurgical or non surgical. Treatmentfailurecanbedue to manyreasonsfrommissedcanaltoiatrogenicperforationwhich has to beevaluatedcarefullybeforeinitiatingthetreatment. Sometimes a clinicianalso has to dealwithinterappointmentfl are upsrequiringprompt and efficientpatientmanagement. Thiscase report describesthe non surgicalmanagementoffailedrootfilledteethwhich had alsobeentreatedsurgically. • Conventionalendodontictreatmentmayfaildue to variousreasons and inadequaterootcanaltreatmentwithpersistentinfectionremaining in inaccessibleareasofthecanalbeingoneofthem
Fig 1: Clinical photo of the patient showing draining sinus Fig 2: Preoperative IOPA Radiograph Fig 3: After Gutta percha removal
Fig 4: Immediate post obturation Fig 5: 12 months recall Fig 6: 24 months recall (decrease in size of periapical lesion is evident)
If root fi lled tooth has failed, there can be fi ve possible treatment options: To review or do nothing, root canal retreatment, root end surgery, extraction followed by implant or referral. Cross sectional studies from different countries including most recent studies clearly demonstrate that more than 30% of all root fi lled teeth in the population are associated with apical periodontitis or post treatment disease9,10,11,12. A general guideline has been given by European Society of Endodontology13 for indications of retreatment, they are; • Teeth with inadequate root canal fi lling with radiological fi ndings and/or symptoms • • Teeth with inadequate root canal fi lling when the coronal restoration requires replacement • • Teeth with coronal dental tissue that is to be bleached
Conclusion • Thereisenoughpotentialforsuccessofprimaryrootcanalfillingbutfactremainsthatclinicians are confrontedwith post treatmentdisease. Endodonticretreatmentcouldbe a suitableoption in caseof a post treatmentdiseasefollowinganendodonticfailure. • Nonsurgicalprocedurescouldlookofminorimportance or insignificantduringretreatment, formanagingsurgicalendodonticfailureespeciallywhenreendodonticsurgeryappearsinevitable. However, with non surgicaltreatmentapproach and adequateapicalandcoronalsealingwecanachievefavourableclinicaloutcomeeven in caseoffailedsurgicallytreatedteeth.