Download
1 / 55
580 likes | 720 Views
GERD LEADS TO RESPIRATORY SYSTEM DİSEASES. Dr. Remziye TANAÇ Ege University School of Medicine Division of Pediatric Allergy and Pulmonology. GERD. GER is reflux of the gastric contents into the esophagus At least one regurgitation in a day 0-3 months period 50%

E N D
GERD LEADS TO RESPIRATORY SYSTEM DİSEASES Dr. Remziye TANAÇ Ege University School of Medicine Division of Pediatric Allergy and Pulmonology
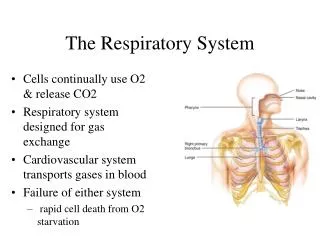
GERD • GER is reflux of the gastric contents into the esophagus • At least one regurgitation in a day • 0-3 months period 50% • In 4th months 67% • 10-12 months period 5% • Decrease after 6-months-old
REFLUX Gastroesophageal Reflux (GERD) • Physiological • Functional • Pathologic (GERD) • Secondary Pharyngolaryngeal reflux (PLR) is to reach up the gastric contents to the upper-esophageal sphincter with no vomiting and retching
GERD Most common extraesophageal symptom is concerning the respiratory system • Bronchial hyperreactivity (infantile wheezing,asthma) • Recurrent pneumonia • Chronic cough • Infantile apnea • Laryngeal diseases • Otitis media • Sinusitis • Adenoidal hyperplasia
GERD and Common Pulmonary Symptoms • Distal esophagus originates from lung pouch embryologically • Vagal nerve innervates distal esophagus and airway • Throughout life ‘association and interaction in thoracal cage’
HISTORY • 12th Century Moses Malmonides ‘horisontal position is harmful for dyspnea’ • 18th Century Rosenstein ‘stomachic cough’ • 1802 Haberden ‘in some people respiration becomes fast and forced after meals’ • 1892 Osler ‘overeating must be avoided’ • 1934 Bray ‘airway obstruction in people who lie down right after meals’ • 1962 Kennedy ‘silent reflux in airway diseases’ • 1970 Barr ‘GERD is one of the causes of bronchial obstruction’ Ped.Clin. Notrh. Am. 50 (2003) 487-502
Prevalence GERD • 40% in general population • Classical reflux symptoms • 40-50% in asthmatic patients • 57% patients have URT symptoms • 43% in chronic cough Not very Clear Clinical Cornerstone 2003, vol.5-4
Prevalence In general: • Pulmonary symptoms 42% in children with GERD • Asthmatic symptoms 60-80% in adults with GERD • Asthmatic symptoms 56-60% in children with GERD Ped. Pulm. Supp. 2004 26: 194-96 J. Pediatrr. 2005 146:s.3-12
Mechanisms of GER • Macroaspiration Chronic laryngitis,recurrent sinusitis,otitis media,recurrent pneumonia,bronchectasis • Microaspiration Chronic cough,bronchospasm • Esophagolaryngeal/Bronchial vagal reflex,local axonal reflex Chronic cough,laryngospasm,infantile apnea,bronchospasm Immunol. Allergy. Clin. N. Am. 28 (2005) 131-148
Macro-Micro Aspiration Theory Acid reflux into the trachea Increase in total lung resistance Decrease in intratracheal pH Induce chemo and sensory receptor-vagal reflex Cough,bronchospazm
Esophagobronchial/Vagal/Local Axonal Reflex • Distal esophagus originates from lung pouch embryologically • Vagal nerve innervates distal esophagus and airway
Gastric contents Regurgitation into esophagus Induced lower esophageal receptor Vagal stimuli (Bronchospasm,cough) Local axonal reflex Esophagus-lung interaction (NO) (Substance P, neurokinin A)
GERD-Reactive Airway Disease (Asthma-Wheezy child)
Association of Asthma and GERD • 30% > 80% • 24% - 77% • 45% - 65% • 50% - 60% J.Poelmans.J.Gut 2005:54:492-99 Harding SM:The Am. J.Med. 2003:15(3A)405-445 Lemaske RF: J.Allergy Clin. Immunol 2006: 117: S.445-61
GERD-Asthma-Risk • 10.000 children 2-18 years of age • 7920 children GERD(-) 7% Asthma • 1980 children GERD(+) 13% Asthma OR :1.9 p<0.001 El Serag H.B. Gastroenterology 2001: 121: 1294-9
Field SK 109 Asthma 125 Control GERD 77% 50% Pul. Find 41% • Harding SM pH monitoring Pul. Symptoms in 151 cases 79% Acidic reflux Fıeld S.K.: Chest 1996: 109: 316-22 Hardig S.M.:Chest 1999: 115: 654-59
Lung Function Test(LFT)-GERD 34 Asthmatic children (2.5-17 years of age) pH monitoring Endoscopy LFT 87% pathologic reflux FEV1/FVC (r = -0.67) Increase of pathologic reflux in severe asthmatic patients Farcau D. Pneumologia 2004 53(3):127-71
Nocturnal GERD-Asthma 77 Asthmatic children (39-170 months of age) More nocturnal GERD in moderate and severe asthma than mild group Cinquetti J.Asthma 2002: 39:135-42
Nocturnal GERD-Pul. Symptoms-PEF Randomised n: 2197 (20-48 years of age) GERD (complains of patient) FEV1-PEFR-BHR Results: GERD in 101 patients - 4.6% Wheezing OR: 2.5 (95% CI) Dyspnea OR:2.8 nGER(+) 5.4% ± 4.2 nGER(-) 4.2% ± 3.5 No change in FEV1 PEF variability p<0.05 Gislason T. Chest 2002: 121: 158-63
GERD-Asthma-Morbidity 2397 children 13-14 years of age Questionnaire: Asthmatics n:296 GERD 19.3% Non- asthmatics n:1510 GERD 2.5% Debley J.S.:Ped.Pulmonol 2006: 41:475-81
Wheezing-GERD • pH monitoring in 190 children 15.8% wheezing • 82 children (Med. age 17.4 months) Recurrent wheezing 21.9% GERD Goldami H. Arq Gastroenterol 2005,42(3)173-2 Karaman O.Indian J.Peditr. 1999, 66(3):351-5
Wheezing-GERD • Non-atopic 25 patients (wheezing+cough) 25 control • 72 ±38.1 months of age • pH monitoring • Therapy for three months with PPI Yüksel H. Respiratory Med.2006, 100;393-98
Therapy of Asthma-GERD Meta-analysis (Adult) 1966-1996 12 studies 326 Patients 8 placebo controlled 3 open 1 untreated control group Result 69% decrease in asthmatic symptoms 62% decrease in antiasthmatics usage 26% increase in morning PEF value Field SK: Chest 1998, 114(1),275-83
Asthma and Therapy of the GERD Prospective (Adult) 30 Patients 73% GERD(+) Medication with PPI for three months Result 20% increase in PEF 20% improvement in asthmatic symptoms Need for 12 week therapy Harding M.S.. Immunol. Allergy. Clin. North Amer.25,2005,131-48
Asthma and Therapy of the GERD Multicentric,double-blind placebo controled 207 Patients Moderate persistant (Adults) PPI 30 mgx2 6 months Decrease in asthma attacks Improvement in life-quality Littner M.R. Chest 2005: 128:1128-35
Asthma and Therapy of the GERD 27 Patients 5-10.5 years of age 59% GERD(+) by Ph Monitoring Medical+surgical treatment Result After 6 months 50% decrease in bronchodilator usage 89% decrease in inhaled steroid usage Khoshoo V.Chest 2003;123:1008-13
Asthma-GERD SURGERY • Meta-analysis 12 studies 417 Patients 90% improvement in GER 80% decrease in antiasthmatics usage 79% decrease in asthmatic symptoms 27% improvement in LFT Field SK.. Chest 1999, 116:760-74
RESULT GERD Leads to Reactive Airway DISEASE (ASTHMA-WHEEZING)
GERD-Recurrent Pneumonia Pneumonia Two or more within one year and/or Three or more at any time
GERD-Recurrent Pneumonia • Patients with neurologic diseases • Children who have congenital malformation related to upper-gastrointestinal system • Healty children with GERD • Increase of GERD incidence in recurrent pneumonia • Improvement in GERD and pneumonia with GERD therapy Euler AR, Byrne WJ, Ament ME. Reccurent pulmonary disease in children:a complication of gastroesophageal reflux.Pediatrics 63(1979),pp47-51 Carre IJ. Pulmonary infections in children with a partial thoracic stomach(hiatus hernia) Arch Dis Child 35(1960)pp481-484
GERD-Recurrent Pneumonia El-Serag (2-18 years of age, children) 1996-2000 n: 10.000 GERD: 1980 Control: 7920 OR: 2.3 CI:1.8-2.9 p<0.0001 El Serag H.B.Gastroenterology 2001:121,1294-9
GERD-Recurrent Pneumonia • Çiftçi E n:788 children 1997-2002 RP:9% GERD:15% Increase risk in <1 year of age • Owaged AF n: 2952 children 1987-1997 RP: 8% GERD:5% Çiftçi E..J.Trop.Pediatr 2003. 49(4) 212-5 Owaged A.F.Arch.Pediatr. 2000.154(8) 850
GERD-Pneumonia-Therapy Chen P n:23 children 3-25 months of age pH monitoring GERD:91% Therapy Improvement:64% Chen. J. Pediatr. Gastroenterology. Nutr. 1991:13(1) 16-22
GERD-Idiopathic Pulmonary Fibrosis 1952 Rabbit,dog acid inhalation - fibrosis Mays EE n:131 Tracheobronchial aspiration n:48 Pulmonary fibrosis in x-ray GERD: 54% Control: 8.5% Tobin RW n:17 Idiopathic pulmonary fibrosis by biopsy n:8 Interstitiel pulmonary disease pH monitoring Acid reflux in 16/17 Acid reflux in 4/8 control Teabeaut J.R.Am.J.Pathol 1952:28:51-62 Glauser FL. Am.Rev.resp.Dis. 1970:126:1119-23 Mays EE Chest. 1976: 69:51-15 Tobin RV. Am.J.Resp.Crit.Care Med.1998:158:1804-08 Raghu G.Am.J.Med. 2003: 115(3A): 60-64
GERD-Cough • Cough 1.Acute 2.Chronic 3.Recurrent • Chronic cough duration >4 weeks in children (3-12) • Chronic cough duration >8 weeks in adults • Recurrent cough: 2 attacks, more than >2 weeks duration in a year or attacks, 1-3 weeks duration in consecutive months • GERD-Cough Non-productive, long duration in the upright position Chang AB Cough 2005 1:7 Vaezi MF. Clin. Cornerstone GERD 2003:5:4: 32-36
GERD-Cough Prevalence In general 21-41% Roka R n:299 GERD:(+) • Pulmonary symptoms 18% (56/299) • Chronic cough 75% (42/56) Poelmans J.Gut 2005;54:1492-99 Roka R. Digestion 2005;7(12):92-6
GERD-Cough-Therapy Poe RH n:183 31% (56/183) GERD-cough 43% (25/56) GERD-unique cause Therapy PPI or PPI+Prokinetic Poe Rh. Chest 2003:123:679-84
GERD-Cough-Therapy Chang AB Meta-analysis n:763 studies 11 Randomised controled studies Adults 8 Children 3 n:383 Chang AB. BMS: 2006:332:11-17
Results: Treatment with PPI is beneficial for GERD related cough in adult patients.Needs more studies for children.
GERD-Infantile Apnea-ALTE Infants respond to laryngeal stimuli as central and/or obstructive apnea But response in children as cough
GERD-Infantile Apnea-ALTE Mc Guirth WF Meta-analysis 1979-2003 99 studies 56 studies (Children) in meta-analysis Prevalence Premature 33-100% Infant in term 25-100% Symptoms control 27-100% Mc Guirth WF. Ped.Clin. North Am: 2003:50: 487-502
GERD-Laryngeal Symptoms-Therapy El Serag HB Placebo controled study PPI for 3 months Improvement in 50% patients Improvement in 10% placebo group El Serag HB.Am.J.of Gastroenterology:2001:(96):1997
GERD-Otitis Media • Pepsin/pepsinogen in the middle ear in 73% children with otitis media • High pepsin/pepsinogen level in 59/65 patients with otitis media • Improvement, after anti-reflux therapy for 11 weeks Judith EC. 2005 Otholaringology 133:357-61 • Poelmans J. Gut 2005:54 1492-1499
Esophagopulmonary and Pharyngolaryngeal Reflux in Children with Pulmonary Symptoms Betül SÖZERİ YENİAY*, Figen GÜLEN*, Sema AYDOĞDU*, Remziye TANAÇ*, Levent MİDYAT*, Fatih ÖĞÜT**,Tayfun KİRAZLI**,Funda ÖZGENÇ*, Raşit V. YAĞCI*, Esen DEMİR* * Ege University School of Medicine Division of Pediatric Allergy and Pulmonology, İzmir ** Ege University School of Medicine Department of Otorhinolaryngology ,İzmir
AIM To evaluate demographic characteristics, follow-up and response to the therapy in children with GERD
METHOD • Outpatients were admitted to Ege University School of Medicine Division of Pediatric Gastroenterology and Hepatology with pulmonary complaints • Diagnosis of GERD: History,scintigraphy,24 hour pH monitoring • Pharyngolaryngeal reflux: Otorhinolaryngologic examination • Statistical analysis: SPSS 10.0 Meanful p<0.05