Download
1 / 77
910 likes | 1.74k Views
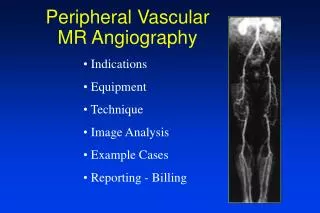
Peripheral Vascular Disease, Angiography - Angioplasty and Surgical Techniques. Dr. Rajdeep Agrawal, MD, DM Interventional Cardiologist & Vascular Interventionist , Sir H N Hospital,Mumbai Breach Candy Hospital Cumballa Hill Hospital. Indications of Angiography in PVD.

E N D
Peripheral Vascular Disease, Angiography - Angioplasty and Surgical Techniques Dr. Rajdeep Agrawal,MD, DM Interventional Cardiologist & Vascular Interventionist, Sir H N Hospital,Mumbai Breach Candy Hospital Cumballa Hill Hospital
Indications of Angiography in PVD • Life style limiting claudication • Critical ischemia / limb threatening ischemia (rest pain, nocturnal pain, non healing ulcer, gangrene • Graft stenosis • High surgical risk • Acute ischemia of lower limb Dr. Rajdeep Agrawal
Arteriogram • Remains the ‘Gold standard’ for vascular evaluation. • Should be done only in patients who have clinical indications for vascular interventions (surgery or angioplasty) • Complications are less than 5% and mortality about 0.025%. • Patients should be well hydraded before and after angiograms, especially diabetics. Dr. Rajdeep Agrawal
Angioplasty -- History • Charles Dotter (1964) • First angioplasty using co-axial catheter • Andreas Gruentzig (1977) • First PTCA using double lumen catheter Dr. Rajdeep Agrawal
Percutaneous Transluminal Angioplasty (PTA) in Peripheral Vascular Disease An over view of the arterial pathologies of the lower limbs and their percutaneoustreatment modalities Dr. Rajdeep Agrawal
Percutaneous Transluminal Angioplasty • A non-surgical technique designed to increase the lumen of the vessel & thus prevent ischemia & its complications • Mechanism Inflated balloon exerts circumferential pressure on the plaque 1. Plaque splitting & disruption 2. Stretching of the vessel wall 3. Compression of the atheroma Dr. Rajdeep Agrawal
Rutherford – Becker classification of PVD Dr. Rajdeep Agrawal
Rutherford – Becker classification of PVD Ankle Brachial Index - > 0.90 – No significant obstructive disease 0.50 to 0.90 – Claudications (Grade I) <0.50 – Limb threatening ischemia (Grade II or III) Dr. Rajdeep Agrawal
Ideal settings for PTA Dr. Rajdeep Agrawal
Percutaneous Transluminal Angioplasty (PTA) in Peripheral Vascular Disease Modalities will include – Angioplasty, Stents, Lasers, Rotablaters, And Thrombolysis Dr. Rajdeep Agrawal
Percutaneous Transluminal Angioplasty (PTA) in Peripheral Vascular Disease Modalities will be treated together or separately in the territories commonly affected by vascular disease Acute arterial obstruction will be treated as a separate issue, where multimodal treatments may come together Dr. Rajdeep Agrawal
Lower Limb Ischemia - Vascular involvement in Diabetic • Aorto illiac relatively spared. • Most of the diseases involves infrainguinal arteries (femoral - popliteal - tibial) • About 60% have involvement of plantar arch and digital arteries. • About 80% have microangiopathy Does not adversely affect the outcome of vascular reconstruction. Dr. Rajdeep Agrawal
Angiography -- Technique • Approach • Femoral / Brachial • Vascular accessusing Seldinger’stechnique • Material / Hardware • 0.035 guide wire • Renal catheter, Simmon’s cath Dr. Rajdeep Agrawal
Seldinger needle & guide wire for introducing an arterial catheter Dr. Rajdeep Agrawal
Arterial Occlusion just above the knee causing claudication of the calf; good collateral circulation Dr. Rajdeep Agrawal
Balloon Catheter for PTA Dr. Rajdeep Agrawal
Contraindications to percutaneous revascularization PTA C/I - Medically unstable (Absolute) - Stenosis adjacent to aneurysm or near an ulcerated plaque (Relative) - (Unfavourable anatomy) Long segment & multi-focal stenosis Long segment Occlusions (thrombolysis) Dr. Rajdeep Agrawal
Percutaneous revascularization PTA Contra-indications (Relative) - If large vessel at ankle is available for bypass - Heavy eccentric calcification - Lesion in essential collateral vessel - Stenosis with thrombus Dr. Rajdeep Agrawal
Percutaneous revascularization Post PTA recurrence are seldom worse than before, does not interfere with the original planned surgery. In 25% Femoro - popliteal PTFE Graft, Popliteal gets occluded when bypass closes Adar etal Dr. Rajdeep Agrawal
Percutaneous revascularization THROMBOLYSIS is an alternate attemptable modality of treatment in PVD Safe if cases are selected properly Cannot be used in all cases. Various methods are used to administer thrombolysis Acute ischemia of lower limb is one area Dr. Rajdeep Agrawal
Percutaneous revascularization Intra-arterial Thrombolysis Restores blood flow Identifies underlying lesion Thrombotic or embolic occlusion Native artery or bypass graft Dr. Rajdeep Agrawal
Percutaneous revascularization THROMBOLYSIS - CONTRAINDICATIONS Absolute -Active internal bleeding Irreversible limb ischaemia Recent stroke, craniotomy Mobile L-V thrombus Dr. Rajdeep Agrawal
Percutaneous revascularization THROMBOLYSIS CONTRAINDICATIONS Relative - H/o GI bleed - Recent major surgery/CPR/Trauma - Diastolic BP >125 mm - DM – Proliferative Retinopathy - Sub acute bacterial endocarditis - Coagulopathy - Post partum state Dr. Rajdeep Agrawal
Percutaneous revascularization Stents: Contra indications - Diffuse aortic disease - Extravasation of contrast after PTA - Non compliant lesion on angioplasty - Diffuse iliac disease - Aortic tortuosity & aneurysm - Diffuse long segment small caliber external iliac or femoral artery Dr. Rajdeep Agrawal
Percutaneous revascularization Stent Complications (10%) • Almost all are minor • Puncture site injury • Distal embolization • Stent dislodgement • Pseudo anemysm formation • Vessel rupture Dr. Rajdeep Agrawal
Percutaneous Transluminal Angioplasty (PTA) in Peripheral Vascular Disease AORTO – ILIAC Percutaneous Transluminal Angioplasty - Optimizes inflow for bypass - Excellent patient tolerance - Short recovery period - No worsening of vascular status – if fails Dr. Rajdeep Agrawal
Percutaneous revascularization AORTIC OCCLUSSIONS • Relatively uncommon • Younger population who smoke • Claudication and impotency • Risk of propagation of clot to renal and mesenteric artery Dr. Rajdeep Agrawal
Percutaneous revascularization ABDOMINAL AORTIC STENOSIS • Isolated - relatively uncommon • More frequent in women with hypoplastic aortas • PTA and Stent can be tried and are useful if the lesions are amenable • Otherwise Grafts can be placed • Even thrombolysis could be attempted with angioplasty • Large thick atherosclerotic lesions could be common Dr. Rajdeep Agrawal
Percutaneous revascularization AORTO – ILIAC STENTING Indications - Residual stenosis > 30% after percutaneous revascularization Or if a gradient >10mm persists Dissection Highly eccentric stenosis Recurrent Stenosis post PTA Iliac artery occlusion Dr. Rajdeep Agrawal
Percutaneous revascularization ILIAC ARTERY STENOSIS PTA • PTA with/without stent • Focal, uncalufied sterosis <5 cm long • Eccentric or calufied sterosis < 3cm long Long segment (>10cm)respond less favorably STENTS • Residual pressure gradient (<5mmHg) or residual stenosis(>30%) • Flow limiting dissection flap • Restenosis (acute or subaiute) Dr. Rajdeep Agrawal
Percutaneous revascularization ILIAC ARTERY OCCLUSIONS • Bilateral – Surgery treatment • Primary stent placement • PTA followed by stent • Thrombolysis followed by stent Dr. Rajdeep Agrawal
Percutaneous revascularization INTERNAL ILIAC STEONSIS • Isolated buttock claudication • Impotence • PTA is the choice Dr. Rajdeep Agrawal
Percutaneous revascularization CFA STENOSIS • Isolated is uncommon without history of injury (eg. Catheterization) • Endarterectomy – choice simple, LA and conscious sedations • Durable than PTA Dr. Rajdeep Agrawal
Ext. Iliac Artery stenosis - before, after dilatation, after stent Dr. Rajdeep Agrawal
Percutaneous revascularization Femoro popliteal - Lesion 3 times commoner than iliac - Occlusions 3 times commoner than stenosis - 80% of the stenosis are <10cm - 20% occlussions < 10cm Dr. Rajdeep Agrawal
Percutaneous revascularization Femoro popliteal - 10 cm upper limit to select cases - Stents disappointing beyond that length of stenosis - Covered (PTFF) grafts have a promise - Over 5 years 15-20% new Femoro popliteal occlussions develop Dr. Rajdeep Agrawal
Narrowed superficial femoral artery before & after dilatation Dr. Rajdeep Agrawal
Percutaneous revascularization Femoropopliteal stenosis: • PTA is less durable than bypass. • Bypass 5 year patency rate is about 80% - Complication of PTA is 10%, surgical repair required in 2% cases Dr. Rajdeep Agrawal
Percutaneous revascularization Femoropopliteal stenosis -Stents useful in proximal Superficial Femoral Artery - Stents – restenosis in distal SFA or popliteal artery due to extrinsic compressions (eg. Addutor canal) is possible - Long term consequences of placing flexible stents across joints is unknown. Dr. Rajdeep Agrawal
Percutaneous revascularization Femoropopliteal occlussions: • Long segment or complete SFA occlusions does not respond well to any widely available endovascular technique • Amplatz thrombectomy catheter – excellent technical access, but long term patency is modest or unknown • Covered stents - results disappointing • Endovascular stent grafts show most promise Dr. Rajdeep Agrawal
Percutaneous revascularization Femoropopliteal occlusions: • PTA is effective for short solitary occlusions, < 10cm long, not involving SFA origins or distal popliteal artery and tenders occlusions <3cm long • Focal occlussions (<2 to 3cm) PTA alone • Long occlussions – Thrombolysis prior to PTA Dr. Rajdeep Agrawal
Percutaneous revascularization Femoropopliteal occlusions: • Upper SFA occlusions – stent if PTA is sub-optimal • PTA long term patency rates may be substantially less than clinical patency rates • Technical failure almost always results from inability to cross the lesion with guide wire. Dr. Rajdeep Agrawal
Percutaneous revascularization Infra-popliteal revascularization - Indications Absence of pedal pulses – minimal or asymptomatic If collaterals are not well developed or limitation of activity results Focal lesions Limited in diffuse disease, If short term patency is desired sufficient to heal superficial ulcerations or amputation sites Dr. Rajdeep Agrawal
Percutaneous revascularization Infra popliteal revascularization – Early results - Not impressive Manipulations - Easier with DSA & road mapping Increased popularity - Safe & Successful Decision with surgeon Inflow lesions Treatment first Dr. Rajdeep Agrawal
Percutaneous revascularization Tibial Artery Obstructions: – Infra popliteal PTA is almost always performed for limb salvage • Short term patency may be sufficient to allow healing of an ischemic ulcer or amputation site or to avoid amputation • PTA is not particularly effective if run-off vessels are not visualized. Liberal Heparin use must to maintain patency Dr. Rajdeep Agrawal
Percutaneous revascularization STENTS RESULTS - Technical success rate – 90-100% - Cumulative 5 year vessel patency – 94% - Clinical success – 93% - (PTA 65% & 70%) Dr. Rajdeep Agrawal
Percutaneous revascularization Infra-popliteal revascularization Indications - Limb threatening Ishcemia (Disabling claudication, Rest pain, Ulcer, Gangrene) - ABI < 0.5 Ischemic rest pain or ankle pressure <60 mm, with or without a non healing ulcer - DM – ABI not useful - calcification Dr. Rajdeep Agrawal
Stent • An expandable metallic helical device which is permanently implanted in the artery. • Mechanism • The prosthesis acts as a scaffold to hold the artery open • Prevents recoil of the vessel • Reduces Restenosis Dr. Rajdeep Agrawal
Newer Techniques Of Angioplasty • Atherectomy • Directional • Percutaneous Rotational • TEC • LASER • Stent Dr. Rajdeep Agrawal
Directional Atherectomy • It excises the atheromatous plaque material into very fine slices which can be retrieved outside body Dr. Rajdeep Agrawal