Download
1 / 61
1.13k likes | 5.44k Views
METERED DOSE INHALER. Presented by: Aarohi Shah M.Pharam. Department of Pharmaceutics and Pharmaceutical Technology L.M. College of Pharmacy. We shall discuss:. Advantages of Nasal Route as systemic delivery Limitations Anatomy of respiratory tract Metered Dose inhalers design

E N D
METERED DOSE INHALER Presented by: Aarohi Shah M.Pharam Department of Pharmaceutics and Pharmaceutical Technology L.M. College of Pharmacy
We shall discuss: • Advantages of Nasal Route as systemic delivery • Limitations • Anatomy of respiratory tract • Metered Dose inhalers design NONPRESSURIZED SYSTEM PRESSURIZED SYSTEM • Manufacturing of Inhalers • Novel Excipients for Inhalation Drug Delivery • Evaluation of MDI as per FDA • Recent innovation in MDI Technology • Application of MDI in Systemic Medication • Market formulations • References
Introduction • The first nasal administration of drugs was primarily employed for local drug effects. • The potential nasal route for systemic delivery was discovered after the observation that nasally administered sympathomimetic and antihistaminic drug for local action has significant systemic effects. • Nasally administered small dose display a rapid absorption that is comparable to intravenously administered drugs.
Advantages of Nasal Route as systemic delivery are: • A non-invasive route • Convenience of administration and amenable to chronic self administration • Avoids first pass metabolism or gastro intestinal tract destruction • A large permeable surface area and rich vasculature availability • Plasma concentration time profile is comparable to intravenous administration • Macromolecules like proteins and peptides can be successfully administered.
Limitations: • Rapid mucociliary clearance • Chances of immunogenic reaction • Inadequate availability of toxicity data for penetration enhancement • Nasal pathology may adversely affect product effectiveness
Columnar epithelium Airway Cilla Mucociliary blanket Anatomy of respiratory tract • This must be understood as a tool for formulating a potential dosage form as an alternative for parenteral route. • Upper and lower respiratory tract with portals of entry being either nose or mouth. • Airway epithelium • The mucous blanket • Various proteins • Nasal pH • Vascularity
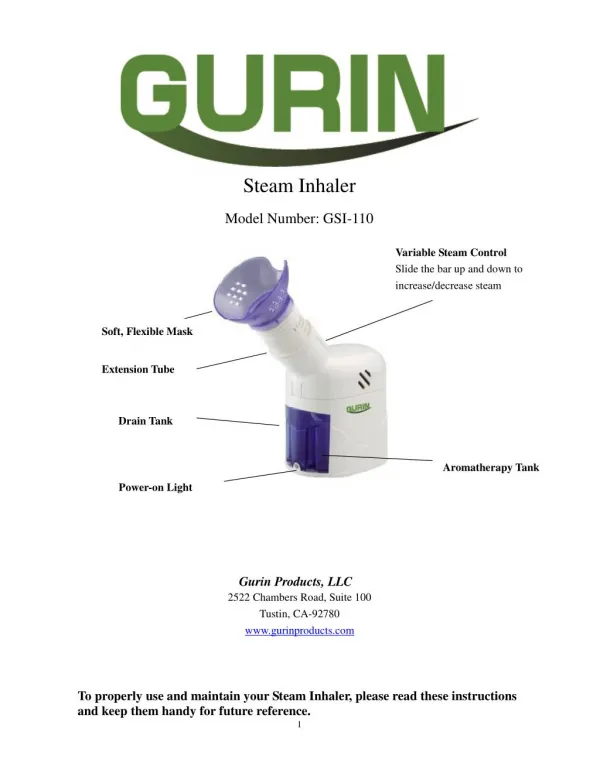
Metered Dose inhalers • It is composed of four essential components: the base formulation (Drug, propellant, excipients, etc.), the container, the metering valve and the actuator (or mouth piece) • The drug is delivered through a valve in a metered volume from a volatile propellant, pressurized container.
Pressure resistant container Liquid solution or suspension Metering chamber Valve stem Actuator Mouthpiece Air inlet Spray jet Metered Dose inhalers
Mainly two types of systems are available • NONPRESSURIZEDSYSTEM (B) PRESSURIZEDSYSTEM
NONPRESSURIZED SYSTEM • Micronised drug is dissolved or dispersed in liquefied propellant (CFC). Before the propellant exits from the atomized nozzle, it is partially (15-20%) evaporated and droplets are broken up by the violent evaporation generating droplets with wide distribution (1-5µm). • But due to alarms raised for stratospheric ozone depletion, a more environment friendly substitutes like Hydrofluoroalkane (HFA) came in light. They have the limitation of poor solvency which can be overcome by addition of co-solvents like ethanol. • Some patients cannot fulfill the co-ordination requirements which is essential for maximum therapeutic benefits, breath actuated powder inhalers are developed.
Powder Delivery System • It’s a versatile system require some degree of dexterity. • It is ozone friendly system requires no CFC to disperse the drug.
A. Unit Dose Device • SPINHALER • ROTAHALER SPINHALER ROTAHALER
B. Multiple Dose device TURBOHALER
B. Multiple Dose device DISCHALER
Formulation • Particle size (< 5µm) • Blended with large lactose particles • PulmoSphere
Manufacturing Process • single dose devices • Multi dose dispense discs
Nebulized Drug delivery Systems • For acute care of nonambulatory, hospitalized patients particularly with co-ordination difficulties. • Not conveniently portable • Solutions or suspensions
Ultrasonic devices • Ultrasound waves - a ceramic piezoelectric crystal
Nebulizer formulation: • The pharmaceutical solution technology - parenteral products • Formulated in water • Co-solvents • pH above 5
PRESSURIZED SYSTEM • Compact pressurized dispensers designed for oral use, which deliver discrete doses of aerosolized medicament by inhalation to the lungs. • The discharged spray undergoes flash evaporation of propellant liquid to produce a finely dispersed aerosol. • The deposition, dependent on the mass of inhaled drug particles which have a suitably small aerodynamic size to be deposited in the required regions of the lungs. • MDIs are apparently simple delivery dosage devices, but in practice very complex.
PRESSURIZED SYSTEM • Consists of five basic components : • Drug concentrate • Liquefied propellant • Container • Metering valve • Actuator
Drug Concentrate Drug powders • Usually suspension, occasionally solution. • Particle size - below 10 m in diameter and mostly below 5 m. • The particle size distribution
Drug Concentrate Drug Suspension • Aggregate irreversibly and deposit on pack surface • The liquid and solid-phase densities • Low solubility in the propellant • Physical stability of the suspension assessed • Surfactants • Presence of minute amount of water.
Drug Concentrate Drug Solution • When the drug is too soluble in propellant. • A co solvent is required and it is usually ethanol. • ethanol concentration (30-50% by wt.) - some disadvantages: Retard evaporation of the spray, which increases oropharyngeal drug deposition and reduce respirable aerosol fraction. Chemical instability of drug Extraction from valve rubber seal
Propellants: • Mainly two types • Liquefied Compressed gases e.g. CFC (chlorofluorocarbons), HCFC(Hydrochlorofluorocarbons), HFA(hydrofluoroalkanes) • Non Liquefied Compressed gases e.g. N2, CO2 • Liquefied compressed gases are preferred over the other one because: • Flash evaporation to give aerosol of fine particle size. • Spray particle size remains constant during pack emptying as inhaler vapor pressure is maintained at constant level. While compressed gas aerosol performance coarsens due to decrease in gas pressure with increase in head space volume.
Propellants: • Currently only three propellants are approved worldwide for MDI products: CFCs 11, 12, and 114 • Now a days, study of propellants of low or zero ozone depletion potential (ODP) is increasing. e.g., HCFCs 22,142b, and 152a Hydrofluroalkanes (HFA) are chlorine-free and are judged to have zero ODP. HFA-134a is an important promising replacent for CFC-12
Containers • Aluminum containers • They are light, strong, break resistant, compact and light proof and significantly inert. • It is prepared by 2 methods (1) Rapid impact “slugging” (2) Precision deep-drawing – Uniform wall thickness, greater strength. • The cans should be capable of withstanding internal pressure of at least 1000kPa (150 psig) without evident distortion. • Glass bottles • Plasticized PVC non bonded coating
At rest During Actuation During release Chamber refilling Discharging Metering Valves • Function • Complex assembly • The valve for suspension products • The typical metering valve
Actuators (Adapter) • Discharge orifice (spray nozzle) and a socket to engage and form a seal with metering valve stem. • A remarkable variety of actuator designs. But, original “band –tube” arrangement with a separate mouthpiece cap remains predominant. • Spacer • The problem of poor patient co-ordination may also be reduced by using breath actuated inhalers, which are activated by the vacuum induced in the inhaler by an adequate inhalation flow rate.
Manufacturing of Inhalers • Mainly 3 methods (1) Cold Filling (2) Pressure Filling (3) Under Cup Filling • Low atmospheric relative humidity should be maintained in filing area in all the methods.
Hot Air Unscrambler II III I The primary steps for all the methods
(1) Cold Filling • The cold filling method is restricted to non-aqueous products and to those products which are not adversely affected by low temperatures in the range of -40°F. • Potential disadvantage include high propellant vapor loss, high cost of refrigerator and humidity control equipment, a possible induction of nonreversible induction of physical changes in formulation.
Chilled Product Concentrate Chilled Propellant Valve IV V VI Cold Filling
Low boiling propellant under pressure Product concentrate Valve IV V VI (2) Pressure Filling
Propellant filling Product concentrate IV V VI (3) Under Cap Filling
The Terminal Procedure • The containers pass through heated water bath heated at 130°F to test for leak and strength of container. • The containers are then air dried, capped and labeled.
Novel Excipients for Inhalation Drug Delivery • Goals : • To expand the range of compound • To increase the clinical benefits obtained from MDI by providing new capabilities like sustained release or greater respirability. • Three primary Application : (1) Suspension aids – to increase the number of compounds that can be prepared as high quality suspensions. (2) Solubilizers – to enable solution formation at high doses. (3) Sustained release agents – to enhance lung residence time of the compound.
Evaluation of MDI as per FDA • Appearance of container and closure system • Microbial Limits • Water or Moisture Content • Dehydrated Alcohol Content • Net Content (Fill) Weight • Drug Content (Assay) • Impurities and Degradation Products • Dose Content Uniformity • Particle Size Distribution • Spray Pattern • Plume Geometry • Leak Rate • Pressure Testing • Valve Delivery (Shot Weight) • Leachables
Particle droplet size analysis • Influence on • High speed flash photography and halography • Laser diffraction size analysis • Phase Droplet Anemometer. • Microscopic analysis with an image analyzer • Cascade Impactor
Particle droplet size analysis • Single Particle Optical Sizers (SPOS) • Disadvantages : Drug particles are not distinguished from excipients. Sampling may not be representative of the whole sample. Assumption: the particles are spherical and of equal density. Light Scattering Counters
Spray pattern • Allows the cross sectional uniformity of the spray to be determined at specified distances away from the pump orifice tip. • In past FDA recommended : with impaction on TLC plates and manual interpretation of spray pattern. • FDA`2003 draft : non impaction method based on laser sheet and digital camera using electronic images and automated analysis.
Plume Geometry • Side view parallel to the axis of the plume of the spray or aerosol cloud to be determined. • In the past, the FDA recommended that plume geometry could be characterized in terms of plume angle, plume width, and plume height using high-speed flash photography. • FDA’s 2003 draft : laser sheet and high-speed digital camera with electronic images. • ImageTherm Developed a SprayVIEW system to simplify the spray and plume geometry. • Plume geometry and spray pattern measurement using SprayVIEW for an aqueous nasal spray.
Reproducibility of Valves • 5 cans are selected from 100 cans supplied. • Actuator is kept in place and container is weighed accurately to ±0.5 mg. • The valve is actuated once, container is reweighed and weight loss is recorded. • Single actuations are repeated and weight loss is measured each time. The time interval between each individual actuation is recorded. • The regions required to be evaluated are of initial actuations and actuations when aerosol container was approximately 10, 30, 50, 70, 95% empty. • All actuations are performed with cans in inverted position.
Loss of prime • It is defined as valve delivery 15% below the mean. • Onset of loss of prime is shown to be dependent on valve design as well as storage position. • Aerosol is weighed to the nearest milligram before actuation. • Aerosol can is placed in inverted position and press the actuator button for 3 seconds to ensure delivery of full dose. • Let the unit stand at room temperature for 1 minute to allow complete evaporation of propellant and the can is reweighed. • Valve delivery for actuation number 5 is considered as representative of the delivery from a fully primed metered dose valve.
Recent innovation in MDI Technology • Research on area of formulations, valves, canisters, elastomers, mouthpieces, etc. • Other Improvements includes, Breathe-actuation technology Ability to deliver therapeutic proteins and peptides Sustained drug delivery Improved shelf life
AERx® SYSTEM : • Sophisticated technology in order to provide precise dosing which includes, • Controlled dose expression • Control of aerosol particle size • Management of the inhalation and delivery • Inhalation and delivery coordination is optimized through a microprocessor-controlled flow sensing system that actuates delivery only at the beginning of the inspiration and within the correct inspiratory flow rate.
ADAPTIVE AEROSOL DELIVERY TECHNOLOGY • Adapts to the patient’s breathing and ensures accurate drug delivery. Detects pressure changes during breathing and constantly adapt to the inspiratory and expiratory flow pattern of the patient. • AAD systems deliver drug until all the preprogrammed dose has been received and gives audible feedback at the completion of treatment, irrespective of the time taken.