Download
1 / 35
370 likes | 1.26k Views
Outpatient Management of Chronic Liver Disease. Quinn Jackson MD Val Carrejo MD October 9, 2019. Objectives. Know how to address abnormal LFTs in the outpatient setting Understand the impact of NASH and how to treat it

E N D
Outpatient Management of Chronic Liver Disease Quinn Jackson MD Val CarrejoMD October 9, 2019
Objectives • Know how to address abnormal LFTs in the outpatient setting • Understand the impact of NASH and how to treat it • Know how to screen patients for and counsel patients with chronic hepatitis C • Know how to treat patients with cirrhosis
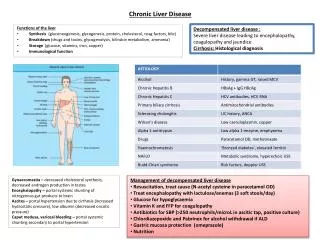
LFTs • Components of liver function tests • Transaminases • Bilirubin • Total protein • Albumin • Alkaline phosphatase • +/- PT/INR
Case 1 • 54 yo man with preDM here for annual physical • BMI 35, BP 145/80 • Labs: • AST 54 • ALT 79 • Bili 0.9 • Total protein 7.9 • Albumin 3.8 • Alkphos 122
Elevated transaminasesMild = < 5x ULN • Common • Alcohol • Non-alcoholic fatty liver • Hepatitis C virus • Less common • Drug induced • Hepatitis B virus • Hemochromatosis • Rare • Wilson’s disease • Autoimmune hepatitis • Alpha 1 antitrypsin deficiency • Extrahepatic causes
Case continues… • A1c 6.4% • cholesterol 250, HDL 35, LDL 150 • HCV, HBV negative • Iron studies and CBC normal • Ultrasound shows increased echogenicity
Non-alcoholic fatty liver disease • About 25% of population has NAFLD • About 2-7% of those have NASH on biopsy • Recommendations for routine screening in high risk populations very different depending on the organization
NAFLD vs Nonalcoholic steatohepatitis • NAFLD = fat accumulation, but no inflammation • NASH = inflammation, cell death and possibly fibrosis • Fibrosis is best predictor of progression to advanced liver disease
Diagnosing fibrosis • Refer to GI Liver biopsy Vibration controlled transient elastography Magnetic resonance elastography Ultrasound has poor sensitivity and specificity! • Limitations to biopsy Technical limitations: liver not uniformly effected, difficulty obtaining specimen Subjective interpretation Complications Cost
Pediatric NAFLD • Most common pediatric chronic liver disease • ~30-40% of children with obesity (BMI > • No clear consensus on screening • AAP recommends biannual screening with liver enzymes in at risk children 9-11 yo (2007) • BMI > 95th% • BMI 84-94th% with risk factors • ALT >22 for girls and >26 for boys
Case 2 • 25 yo woman with history of alcohol use disorder and opiate use disorder presents for buprenorphine induction • Labs: • AST 62 • ALT 84 • Bili 1.0 • Total protein 9.1 • Albumin 3.2 • Alkphos 95
Hepatitis C • Leading cause of liver related mortality in the US • Estimated 2.4 million people living with HCV • Injection drug use most common mode of transmission
Screening • USPSTF Grade B • One time screening for all adults born 1945-1965 • Periodic screening for high risk • Current or past drug use (IV and intranasal) • Blood transfusion before 1992 • Hemodialysis • Incarceration • Unregulated tattoos • New draft statement in public comment phase for screening all adults
Treatment • Oral direct acting antivirals since 2013 • Treatment recommended for all patients unless life expectancy less than 1 year due to non-HCV related cause • Cure = undetectable RNA levels 8-12 weeks after completion of treatment
Counseling • Risk of sexual transmission • Risk of transmission with exposure to blood • Razors, toothbrushes, minor cuts, etc. • Not transmitted from kissing, sharing food or utensils, sharing drinks • People who use drugs (PWUD): Harm reduction! • Syringe exchange, labeling works (“mine”), use own needles, straws and pipes, clean cottons • +/- bleaching works
Case 4 • 65 yo woman with history of alcohol use disorder and diabetes comes into clinical for general follow up • Exam • Red face and palms • Distended abdomen • Bilateral pitting edema
Cirrhosis • Extensive fibrosis with formation of regenerative nodules • Destruction of functioning hepatocytes
Clinical Diagnosis • Spider nevi • Central arteriole, blanchable, refills from center outward • Ascites • Platelets less than 160 • Albumin less than 3.8 • Confirmed with consistent imaging or biopsy
Clinical diagnosis • Jaundice • Sclera under eyelids or mucosa under tongue • Palmar erythema • Actually on thenar and hypothenar eminence
Complications • Malnutrition • Hypotension • Portal hypertension and Varices • Hepatocellular carcinoma • Encephalopathy • Ascites and SBP
Monitoring and HCM • Normotensive to Hypotension • Deescalate medications to keep MAP >82 • Protect the liver! • Hep B and Hep A vaccination • Alcohol cessation • Endoscopy for varices screening/monitoring • Ultrasound for HCC screening
Medications • Safe • Statins • Baclofen • Acamprosate • NOT safe • Disulfuram • Naltrexone • NSAIDs • Use caution • Acetaminophen • Metformin • PPIs
Alcohol and Liver Disease • Chronic injuries to the liver are synergistic • Alcohol plus viral plus obesity • Alcohol use worsens outcomes for all types of chronic liver disease
Board Questions • 52 yo man sees you for a routine health maintenance exam. He does not take any medications, does not drink alcohol, and is feeling well. Physical exam is normal with exception of BMI of 33. Labs reveal mild elevations in AST and ALT, which remain elevated 2 months later. Hepatitis B and C are negative. Which of the following labs should be ordered to further evaluate this patient? • A) Serum ferritin • B) Serum phosphorus • C) Alpha fetoprotein • D) Carcinoembryonic antigen • E) Serum electrophoresis
35 yoman with no known past medical history and normal physical exam. He smokes half a pack of cigarettes daily and has 3-4 beers per week. Reports past intranasal cocaine use. BMI of 37. A comprehensive metabolic panel reveals ALT of 84 and AST of 30. Hepatitis B surface antibody positive. There is no family history of liver disease. These lab findings are consistent with which of the following? • A) Hepatitis B • B) Hemochromatosis • C) Gilbert syndrome • D) Alcoholic liver disease • E) Nonalcoholic fatty liver disease
67 yo woman with history of hepatitis C comes to see you to establish care. She is on furosemide, spironolactone and lisinopril. Her examination reveals blood pressure of 101/62, multiple spider nevi, distended abdomen and thin extremities. Liver function tests are normal. Platelets are 90K. You should do all of the following except: • A) Vaccinate for hepatitis A • B) Ultrasound of liver • C) Discontinue lisinopril • D) Refer for screening endoscopy • E) Discontinue spironolactone
References • Alcohol Use in Patient with Chronic Liver Disease. Fuster, D. and Samet, J. NEJM, 2018, 379(13): 1251-1261 • Causes, Pathogenesis and Treatment of Nonalcoholic Steatohepatitis. Diehl, A. and Day, C. NEJM, 2017 , 377(21): 2063-72. • Diagnosis and Management of Non-alcoholic Fatty Liver Disease: JAMA Clinical Guideline Synopsis series. Paul,S. and Davis,A. JAMA, 2018, 320(23): 2474-75. • Does This Patient with Liver Disease Have Cirrhosis?: JAMA Rational Clinical Exam series. Udell, J et al. JAMA, 2012 (corrected 2018) 307(8): 832-42. • Draft Recommendation Statement: Hepatitis C Virus Infection in Adolescents and Adults: Screening. United States Preventive Service Task Force. https://www.uspreventiveservicestaskforce.org/Page/Document/draft-recommendation-statement/hepatitis-c-screening1 Accessed Sept 23, 2019
References • Hepatitis C Basics for People Who Use Drugs. Harm Reduction Coalition. https://harmreduction.org/hepatitis-c/hcv-basics/ Accessed Sept 22, 2019. • Hepatitis C Questions and Answers for Health Professionals. Center for Disease Control and Prevention. https://www.cdc.gov/hepatitis/hcv/hcvfaq.htm#e1. Accessed Sept 22, 2019. • Management of Hepatitis C in 2019. Marks, K. and Naggie, S. JAMA, 2019, 322(4): 355-56. • Mildly Elevated Liver Transaminase Levels: Cause and Evaluation. Oh, R. et al. American Family Physician, 2017, 96(11): 709-715. • Nonalcoholic Fatty Liver Disease. Fusillo, S. and Rudolph, B. Pediatrics in Review, 2015, 198(36): 198-206
References • Nonalcoholic Fatty Liver Disease: A Challenge for Pediatricians. Nobili, V. et al. JAMA Pediatrics, 2015, 169(2): 170-76. • Screening for Hepatitis C Virus Infection in Adults: USPSTF Recommendation Statement. Moyer, V. et al. Annals of Internal Medicine, 2013, 159: 349-57. • Treatment of Patients with Cirrhosis. Ge, P and Runyon, B. NEJM, 2016, 375(8): 767-777 • Use of Liver Imaging and Biopsy in Clinical Practice. Tapper, E. and Lok, A. NEJM, 2017, 377(8): 756-68.