Download
1 / 22
220 likes | 517 Views
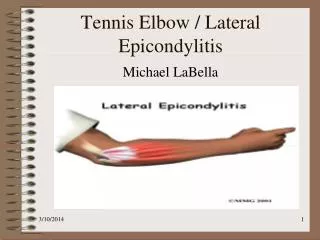
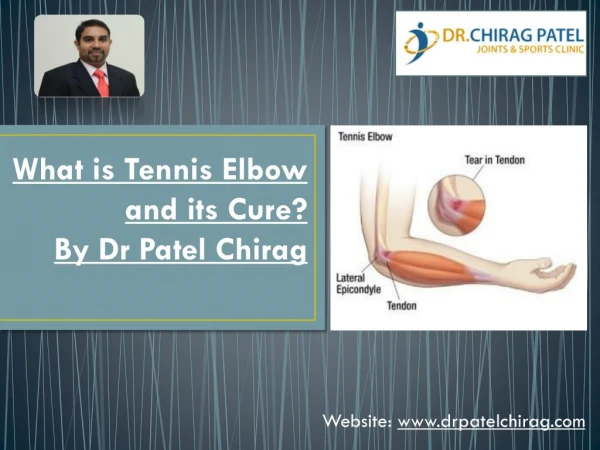
What is Tennis Elbow?. What is Tennis Leg?. Tennis Leg. Tennis leg is a clinical condition first described by Powell in 1883. Tennis Leg. The pathogenesis of this condition has been debated since Powell first described it in 1883

E N D
Tennis Leg • Tennis leg is a clinical condition first described by Powell in 1883
Tennis Leg • The pathogenesis of this condition has been debated since Powell first described it in 1883 • For several years, tennis leg was attributed to a rupture of the plantaris tendon. • More recently, most investigators have implicated a rupture of the medial head of the gastrocnemius muscle at the musculotendinous junction
Tennis Leg • It is an entity that typically occurs in middle-aged persons
Tennis Leg • Injury incurred with extension of the knee and forced dorsiflexion of the ankle .
Tennis Leg • mainly sports-related
Tennis Leg • tennis leg also commonly results from daily activities, such as running to catch a bus or climbing stairs.
Tennis Leg • Sudden pain is felt in the calf, and patients often report a “pop” in the calf or a feeling as though someone has kicked the back of their leg.
Tennis Leg • Usually, there is localized swelling and a bruise often develops. • The injured area is very tender to touch. • The athlete is able to ambulate only with an altered gait pattern that; is characterized by walking on the toes to prevent upward bending of the ankle which would stretch the injured area and afflict further pain.
Tennis Leg • Signs and symptoms of the injury are obvious. A sharp sudden pain that may be described as “it felt like I was shot in the leg” is often reported.
Tennis Leg • Substantial pain and swelling usually develop during the following 24 hours.
141 Patients Studied • US findings in 141 patients referred with a clinical diagnosis of tennis leg were retrospectively reviewed by means of consensus of two radiologists. • Images were analyzed with respect to the integrity of the lower-leg musculotendinous units, presence of fluid collection, and deep venous thrombosis.
141 Patients were Studied • partial rupture of the medial head of the gastrocnemius muscle at or no more than 2 cm from the myotendinous junction, without rupture of the plantaris tendon, was identified in 94 patients (66.7%)
141 Patients were Studied • Of these 94 patients, 59 (62.8%) had associated fluid collection between the medial head of the gastrocnemius muscle and the soleus muscle
141 Patients were Studied • Fluid collection between the aponeuroses of the gastrocnemius and soleus muscles, without US evidence of rupture of the triceps suraemusculotendinous unit, was evident with US in 30 patients (21.3%)
141 Patients were Studied • Rupture of the plantaris tendon was seen in two patients (1.4%) at the middle third of the leg (
141 Patients were Studied • partial rupture of the soleus muscle was seen in one patient (0.7%). • Deep venous thrombosis was seen in isolation in 14 patients (9.9%) and in association with another finding in seven patients (5.0%)
Plantaris Muscle • Together with the gastrocnemius and soleus muscles, it forms the triceps surae muscle • The plantaris consists of a small muscle belly with a thin, long tendon • inserting on the calcaneusanteromedial to the Achilles tendon. In some cases, it fuses with the Achilles tendon. • The plantaris muscle, like the gastrocnemius muscle, spans two joints: the knee and the ankle. • Cadaveric studies have revealed that the plantaris muscle is absent in 7%–20% of limbs. • When absent on one side, it is absent in the contralateral side in 67%
Treatment • The treatment of this condition is usually conservative, with elevation of the lower extremity, application of ice, and use of supportive elastic dressings.
Treatment • The athlete should be given crutches and not bear weight
Treatment • Surgical treatment (fasciotomy) is indicated only when an associated compartmental syndrome has complicated the evolution of the symptoms and signs