Download
1 / 29
290 likes | 358 Views
Explore clinical features and diagnostic procedures related to gastrointestinal sensations, dysphagia, and related disorders. Learn about Achalasia, Zenker’s Diverticulum, and GERD.

E N D
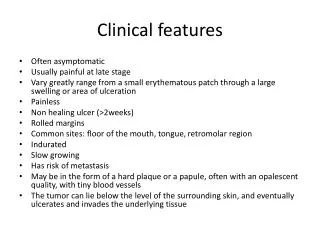
Sensation of “sticking” or obstruction of the passage of food through the mouth, pharinx or the esophagus. • Dysphagia (D) should be distinguished from other symptoms related to swallowing. • Aphagia – complete esophageal obstruction – medical emergency • Difficulty in initiating a swallow occurs in disorders of the voluntary phase of swallowing • Odynophagia(O) painful swallowing • Frequently O + D occur together
Globus hystericus – sensation of a lump lodged in the throat. • Phagophobia – fear of swallowing • Refusal to swallow: hysteria, rabies, tetanus, pharyngeal paralysis • Feeling of fulness in the epigastrium after a meal or swallowing air ≠ dysphagia
Approach to the patient with D • History – diagnosis in 80% of patients • The type of food – useful information • Difficulty only with solids – mechanical D; the lumen is not severely narrowed (drinking liquids through the narrowed area force the impacted bolus) • Advanced obstruction – D with liquids/solids • Motor D (achalasia + esophageal spasm) total D from the onset • Scleroderma – D to solids unrelated to posture/liquids in the recumbent, but not in the upright posture
Peptic stricture developes – D became more persistent • The duration and course of D – helpful in diagnosis • Transient D of short duration – inflammatory process • Progressive D of a few weeks to a few month’s duration – carcinoma of the esophagus • Episodic D to solids of several years duration – benign disease of the esophageal ring • Associated symptoms provide important diagnostic clues • Nasal regurgitation • tracheobronchial aspiration + swallowing hallmarks of pharingeal paralysis/tracheoesophageal fistula
ACHALASIA ZENKER’S DIVERTICULUM GERD laryngitis secondary GER • Tracheobronchial aspiration unrelated to swallowing • Severe weight loss – carcinoma • Hoarseness – precedes/following D → • larynx primary lesion, • recurrent laryngeal nerve caused by extension of esophageal carcinoma
Prolonged nasogastric intubation • Ingestion of caustic agents • Previous radiation therapy causes of esophageal strictures • Hiccups suggest lesion in the distal portion of esophagus • Unilateral wheezing + D→ mediastinal mass → esophagus/large bronchus • Chest pain + D → esophageal spasm (motor disorders) • Prolonged history of heartburn and GER preceding D → PEPTIC STRICTURE • Odynophagia: candidal, herpes esophagitis suspected • AIDS → esophagitis
PHYSICAL EXAMINATION • Important in motor D due to skeletal muscle, neurologic, oropharyngeal diseases • Neck → thyromegaly/spinal abnormality • Careful inspection of the mouth + pharynx → lesion → pain/obstruction • Changes in the skin, extremities • Scleroderma • Collagen vascular diseases • Mucocutaneous diseases(pemphigoid,epidermolysis bullosa) • Pulmonary complications – acute aspiration pneumonia • Metastatic diseases to limph nodes and liver
DIAGNOSTIC PROCEDURES • BARIUM SWALLOW + CINERADIOGRAPHY • ESOPHAGOGASTROSCOPY+BIOPSY+EXFOLIATIVE CYTOLOGY • ESOPHAGEAL MOTILITY • PH-METRY • ESOPHAGEAL IMPEDANCE • ECHOENDOSCOPY • COMPUTER TOMOGRAPHY • MAGNETIC RESONANCE
ANOREXIA (A) • In diseases of GIT and liver • It may precede the jaundice in Acute Hepatitis • Prominent symptom in gastric carcinoma • A ≠ SITOPHOBIA (fear of eating because of subsequent abdominal discomfort) • A may be a prominent feature of extraintestinal diseases • Chronic pain from any source →loss of appetite • In cancer, A results from anxiety, pain, decreased sense of taste + smell, effects of the tumor on the GIT (tumor necrosis factor)
Medications:Antihypertensive Diuretics Digitalis Narcotic analgesics • Psychogenic disturbances – A nervosa • Congestive heart failure/Respiratory failure • Endocrinopathies/hyperparathyroidism, Addison’s disease Mechanism of hunger + apetite Food intake is reglated by 2 hypotalamic centers: • Lateral “feeding center” • Ventromedial “satiety center” • CCK (brain gut peptide) – satiety effect
NAUSEA AND VOMITING • common manifestations of many organic/functional disorders • ACUTE ABDOMINAL EMERGENCIES leads to “SURGICAL ABDOMEN” • acute appendicitis • acute cholecystitis • intestinal obstruction • acute peritonitis • DISORDERS OF THE ALIMENTARY TRACT • peptic ulcer • GI motility disorders • Postvagotomy • Diabetus • Idiopathic gastroparesis • Liver, pancreas, biliary tract disorders
VIRAL, BACTERIAL, PARASITIC INFECTIONS OF THE IT • ACUTE SYSTEMIC INFECTIONS – young children→ FEVER • CENTRAL NERVOUS SYSTEM DISORDERS • neoplasms • encephalitis • Meniere’s disease • migraine headaches • acute meningitis • ACUTE MYOCARDIAL INFARCTION • CONGESTIVE HEART FAILURE • CANCER – patients terminally ill • METABOLIC + ENDOCRINOLOGIC DISORDERS • HYPEREMESIS GRAVIDARUM
SIDE EFFECTS OF DRUGS: • digitalis • morphine • chemotherapeutic agents • ingestion of a toxic (food poisoning) • PHYCHOGENIC VOMITING:anorexia nervosa, bulimia Relationship of vomiting (V) to eating → diagnostic • V that occurs in the morning: pregnancy, uremia • Alcoholic gastritis – early-morning retching, emesis • V shortly after eating → peptic ulcer + pylorospasm • V 4-6 h after eating → pyloric obstruction, esophageal disorders (achalasia, Zenker’s diverticulum) • Relief of abdominal pain with vomiting→ peptic ulcer • rarely satiety→ gastroparesis
INDIGESTION • represents a challenging + difficult diagnostic problem because of its nonspecific nature • Abdominal pain – evaluated with Rx, imaging studies of the esophagus, stomach, small intestine, colon, pancreas,biliary tract. • ESOPHAGOGASTROSCOPY • ERCP • COLONOSCOPY • Empiric trials of antiacids, H2-Rblocking drugs or sucralfat are used in patients < 40 years with epigastric pain • SDE- persistent symptoms despite therapy/recur soon after discontinued therapy
H pylori patients – oral AB 7 days after SDE + biopsy • Excessive gas, bloating, distension, flatulence → questionary: dietary preferences relation of symptoms to specific foods • Elimination of milk, legumes from the diet → confirmatory NONULCER DYSPEPSIA-disturbances of GI motility Esophagus-Substernum,epigastrium-Peptic esophagitis,stricture,esophageal spasm,carcinoma Stomach-Epigastrium-Gastritis,gastric ulcer,carcinoma Duodenum1+2-Epigastrium-Duodenal ulcer Small intestine-Periombilical-Enteritis,lymphoma,obstruction Gallbladder,pancreas,liver-Epg.,right,left upper qt.,back-Cholelithiasis,Pancreatitis,Hepatitis,Cirrhosis,carcinoma.
Colon-below umbilicus-UC,carcinoma,obstruction • Non-ulcer dyspepsia-20-30% of population Helicobacter pylori + chronic gastritis • Heartburn (pyrosis): • reflux of acid/bile into the esophagus • after a large meal • in supine • Fluid in the mouth: salty (“water brash”) sour (gastric contents) bitter green/yellow (bile) • After citrus fruit juices, drugs (alcohol, aspirin)
Food intolerance • Carcinoma -discomfort for solids • Citrus ↓ pH → peptic ulcer, esophagitis • Deficiency of a specific enzyme (lactase-milk) • abdominal cramps • distention • diarrhea • flatulence • Allergic reactions – urticaria, angioedema, asthma • Toxic effects – gluten in celiac sprue • History of fatty food intolerance or distress after spicy foods is commonly in patients with indigestion
ERUCTATION (BELCHING) • Chronic anxiety • Rapid eating • Drinking carbonated beverages • Gum chewing • Postnasal drip • Poorly fitting dentures • 20-60% of intestinal gas is swallowed air • gastric bubble syndrome • splenic flexure syndrome-fullness in left upper quadrant with radiation to the left side of the chest • ↑ tympany + air in the splenic flexure of the colon on a plain abdominal radiograph
GASEOUSNESS, BLOATING, FLATULENCE • Motility disturbances • Fermentative action of intestinal bacteria or carbohydrates and proteins within the lumen CO2 small intestine → HCl, ingested fatty acids are neutralized by bicarbonate 1/3 of adults produce methane in the colon unrelated to food ingestion • Ex. Beans contain oligosaccharides that can’t be split by intestinal mucosal enzymes, but are metabolised by colonic bacteria • Increased intraluminal gas may result from abnormal bacterial colonization of the small intestine or infection with Giardia lamblia
WEIGHT GAIN • CAUSES OF OBESITY • Excess caloric intake • Cushing’s syndrome • Hypothyroidism • Hypogonadism • Insulin-secreting tumors • Cranyopharyngioma (disense of hypotalamus) WEIGHT LOSS • more often a diagnostic problem than weight gain, a sign of serious organic illness.
DIABETES MELLITUS • ↑ insulin-dependent form (insulin deficiency + ↑ glucagon) cause accelerated proteolysis and lipolysis → net energy state is catabolic • Weight loss is associated with increased food intake ENDOCRINE DISEASE • THYROTOXICOSIS • PHEOCHROMOCYTOMA → catecholamine release • PANHYPOPITUITARISM • ADRENAL INSUFFICIENCY → cortisol deficiency
GASTROINTESTINAL DISEASE • Inflammatory bowel disease • Parasites • Esophageal strictures • Chronic peptic ulcer • Pernicious anemia • Cirrhosis liver INFECTION • Tuberculosis • Fungal disease • Amoebic abcess • Subacute bacterial endocarditis • HIV • Cause: inflammatory cytokines
MALIGNANCY • GIT • Pancreas • Liver • Lymphoma • Leukemia PSYCHIATRIC DISEASE • Schizophrenia • Depression RENAL DISEASE
Upper GI Bleeding Peptic ulcer Gastritis Varices Mallory-Weiss syndrome Gastric carcinoma Lymphoma Polyps Dyscrasias, vasculitis Lower GI Bleeding Anal + rectal lesions Colonic lesions, carcinoma, angiodysplasia, UC, ischemic colitis Diverticula Meckel’s congenital distal ileum – 2% GASTROINTESTINAL BLEEDING- etiology -
HISTORY • Ulcer disease • Recent heavy use of alcohol/AIND → erosive gastritis, esophageal varices • Aspirin → gastroduodenitis peptic ulceration bleeding • Acute onset of bloody diarrhea → IBD
PHYSICAL EXAM • DERMATOLOGIC • telangiectasia Osler-Weber-Rendu • perioral pigmentation of Peutz-Jeghers • diffuse pigmentation hemochromatosis • spider angiomata • gynecomastia • testicular atrophy • jaundice • ascites • hepatosplenomegaly – HTP → varices • abdominal mass → malignancy • RECTAL EXAMINATION → local pathology color of the stool
LAB STUDIES • Hb, Ht, WC, IP • Radiography of the abdomen → perforation, ischemia is suspected • Repeated evaluation of the lab data-clinical course of the bleeding. • CONSTIPATION and DIARRHEA • -functional and organic disorders • IRRITABLE BOWEL,colonictumors,IBD,mucosal disorders ,sprue,pancreaticinsufficiency,postgastrectomy,endocrinediseases,habitual.
DIAGNOSTIC • ENDOSCOPY:diagnostic treatment: coagulation Nd-YAG laser, elecrocautery, sclerotherapy of varices • ANGIOGRAPHY:localise the site of bleeding intraarterial infusions of vasoconstrictor agents/vasopressin • COLONOSCOPY: GI bleeds, polypectomy/electrocoagulation • Barium enema – limited role • Arteriography– active blood loss > 0,5 ml/min • Bleeding scans