Download
1 / 29
290 likes | 321 Views
Common Triage Problems. Overview. Labor Evaulation Prodromal Labor SROM Decreased Fetal Movement Bleeding Abdominal Trauma/Falls Pre- eclampsia Abdominal Pain Preterm Labor Preterm Premature Rupture of Membranes. Labor Evaluation.

E N D
Overview • Labor Evaulation • Prodromal Labor • SROM • Decreased Fetal Movement • Bleeding • Abdominal Trauma/Falls • Pre-eclampsia • Abdominal Pain • Preterm Labor • Preterm Premature Rupture of Membranes
Labor Evaluation • Always get a history, don’t rely only on prenatal record!!! • Review prenatal, and ask the patient as well • Take HPI • Timing of Contractions • Any vaginal bleeding? (ie: spotting, bleeding with wiping, frank bleeding) • Any fluid gush/leaking? • Fetal Movement? Has it changed? • What was last vaginal exam in office? (Note date and dilation)
Labor Evaluation • What is Labor? • Labor is painful contractions causing cervical change over time • Do SVE (unless contraindicated) • You need to prove there is change, everyone should get checked if you think they are in labor. This is also why you need to know what the patient was dilated to in clinic • Labor evaluations take TIME! You need to prove there is change
Labor Evaluation • You have checked the patient, now what? • Give the patient a chance to change, again remember, this evaluation can take time. • Re-check in 1-2 hours • If no change, consider walking the patient. If on recheck there is cervical change Admit • If no change Home after Reactive NST
Prodromal Labor • Patient is miserable • Contractions seem painful and frequent but NO cervical change • Main problem= patient exhaustion • Treat like a labor evaluation • If going home, encourage bath, offer Ambien 5-10mg or Hydroxyzine for sleep • If you cannot send patient home you can admit for therapeutic rest • Morphine sleep-10-15mg IM MSO4 +/-IVF
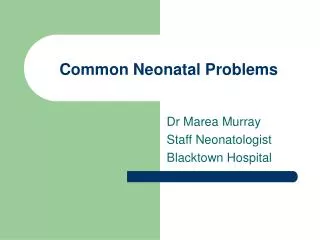
SROM/PROM • Spontaneous Rupture of Membranes /Premature Rupture of Membranes • Leaking fluid – May be the dramatic big gush or slow leak (think peeing your pants) • Do SSE and look for: • Pooling, • Ferning • + Nitrazine • AFI may help in certain circumstances • In some places you can use Amnisure
Graves Speculum Pederson Speculum Sterile Speculum Exam(SSE)
SROM • Verify GBS status and if SROM confirmed, start antibiotics immediately if GBS+ • If still unsure of rupture after SSE, re-examine after 1 hr. • If the patient is NOT in labor, but ruptured (PROM) Check with attending, some will want SVE others may not.
Decreased Fetal Movement • Get a good history from patient • Length of time of no FM and find out how she has been monitoring this • Place of monitor • Await reactive NST (if>32wks). • Reassuring if <32wks. • Doptones ok if <24wks—reassurance. • If non-reactive, may need to do BPP (call Senior)
Fetal Demise • If no heartbeat detected • If the RN is NOT getting a heartbeat and you cannot find it by US…CALL YOUR SENIOR RESIDENT! • Call attending immediately! • You should not typically as an intern being delivering the diagnosis of demise
Fetal Demise • Keep in mind • The ultrasound used for FHT will pick up an adult heart rate on the strip in a demise • This looks like a FHR tracing but with bradycardia. If in doubt, take maternal pulse, do US with M-mode (Ask Senior to help)
Fetal Demise • Keep in Mind • There are patients who will come into triage who are NOT pregnant but say they are (pseudopsychiasis) • These patients may often need psychiatric assistance • You may need to consider having security on floor in this instance as this can cause significant problems with FOB and these patients are at higher risk for infant abduction
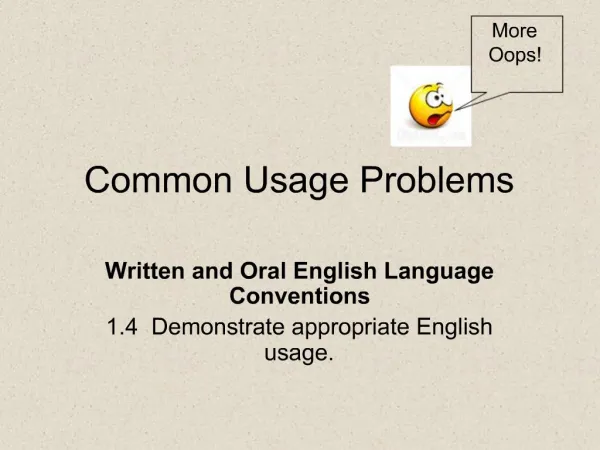
Bleeding • Always consider gestational age and nature of bleeding • 2nd vs 3rd trimester • Painful vs. Painless Bleeding • Almost always perform SSE • Almost never check patient before SSE. • Only exception is placenta previa • Check with attending as to preference. Best to hold on SSE and admit for a formal US. Do bedside US first to look at placenta position
Bleeding • Quantify amount of VB • If patient unstable or NRFHT’s she may need emergent or crash C/S • Remember, patients with abruption can deliver fast – there are times to do a SCE • Abruptions does not always equal C-Section
Bleeding • Common Etiologies: Abruption, Placenta Previa, Bloody Show, Laceration, Friable Cervix • Verify mothers Rh status, T&S • On SSE: use rectal swabs, clean out and look all around, see if active bleeding from os vs friable cervix – may want sponge stick available. • Abruption Labs: CBC, KB, fibrinogen(<200 concern) and T&S vs. draw and hold • If mother Rh-, ad KB shows >15cc fetal cells need to give Rhogam(300mcg full dose) • Bleeding often associated with preterm labor / PPROM
Placenta Previa Placenta Abruption Bleeding
Abdominal Trauma/Falls • Was there abdominal trauma or not? • This may dictate the length of monitoring • If no or limited abdominal trauma, the fetus needs to be monitored for 4 hours continuously. • If contractions, or FHR abnormalities, direct abdominal trauma • 24hrs of monitoring indicated. • General management: • Treatment priorities directed toward injured pregnant woman as they are for non-pregnant patients. First stabilize the mother.
Abdominal Trauma/Falls • Physical exam to look for fractures/abrasions • Verify Rh status • If Rh-, obtain KB • Sometimes patient needs to go to ER for further evaluation ( or re-evaluation) after fetal status shown to be stable. • Remember we don’t fix fractures, gun shot wounds, etc.
High Blood Pressure • History is important • Timing of blood pressures • Gestational age • Is it Gestational HTN, pre-eclampsia, or just an isolated elevated BP? • Have RN take serial BP’s
High Blood Pressure • Characterize symptoms • Get a good history (Is there an echo in here?) • Headache • N/V, Epigastric or RUQ pain, • New swelling, weight changes • Is HA different from normal HA? History of migraines? Does it go away with Tylenol? • Send Labs if indicated • Pro/Cr Ratio • Pre-Eclampsia Panel
Pre-eclampsia • Consider pre-eclampsia panel and CBC: • AST, ALT, BUN, Cr, Uric Acid, LDH • Look at prenatal for baseline BP’s • If prior than 20wkssuspect CHTN • Work-Up Options • Inpatient Monitoring with 24hr urine protein or Pro/Cr ratio, formal US • Send home with precautions and a 24hr urine jug, close f/u plan with primary OB.
Abdominal Pain • Have a broad DDx: • Gallstones, Kidney stones, appendicitis, Gastroenteritis, Hepatitis, Crohn’s, IBS, Cystitis or Pyelo, hydronephrosis, Pancreatitis, adnexal mass, Round Lig pain, pre-eclampsia or HELLP • Normal pains and discomfort of pregnancy
Abdominal Pain • Work Up • Labs • UA, CBC, lytes, LFT’s, amylase, lipase? • Imaging • US to evaluate upper abdomen, renal US • CT scan acceptable if necessary and indicated • MRI safe • Admission • Be open to the need to admit for 23hr obs, pain meds, further workup.
Preterm Labor • Symptoms can be very subtle • back pain, nausea, “just don’t feel right”, menstrual-like cramps, spotting. • “Spec before you check” • Perform SSE first and get: • GBS (rapid), GC/Chlamydia, wet mount, nitrazine and ferning slides, UA, • FFN (attending dependent) if 24-34wks and nothing per vagina x 24hrs.
Preterm Labor • OK to perform SVE after SSE • Place patient on the monitor • Consider US for position, fluid and growth • Main question: Are they changing their cervix, do they need tocolytics to get through the steroid window. • Same examiner checking over 1-2hrs
Preterm Premature Rupture of Membranes (PPROM) • SROM<37wks confirmed • Admit • Get GBS • Ultrasound for position and EFW • If <34wks, give steroids • Start Amp/Erythro IVx48hrs then Amox/Erythro POx5days for latency. • Daily NST • Deliver at 34 0/7
Golden Rules of Triage • If in doubt, ask for help and guidance • The Labor and Delivery RN’s know more than you do (Seriously) • If SCE feels funny, it’s probably breech • Ask for help • Signs and symptoms of both pre-eclampsia/HELLP and PTL can be very subtle • Ask for help • Resist pressure to move patients out quickly. • Ask for help • Think through your assessment and plan before calling the attending • Ask for help • We all make mistakes, learn from them