Download
1 / 23
300 likes | 414 Views
Learn about the risk factors, clinical features, diagnosis, and treatment options for Giant Cell Arteritis (GCA), an inflammatory disease affecting blood vessels, predominantly in individuals over 50 years old.

E N D
What are the risk factors for GCA? • Increasing age • Women affected more often than men • More common among whites, people of Nordic or Northern European background, others residing in Northern latitudes • Genetic markers: HLA-DRB1*04 (alleles 04:01, 04:04) and non-HLA gene polymorphisms (PTPN22) • Current smoking or history of smoking • Possible risk factor: varicella zoster virus
What are the characteristic clinical features of GCA? • Common features related to vascular injury (30%-80%) • Headache • Scalp tenderness • Jaw claudication • Less common features related to vascular injury (<20%) • Ocular symptoms, blindness • Painful dysphagia, respiratory symptoms • Limb claudication • Absent or asymmetrical pulses continuted…
Infrequent features related to vascular injury (<5%) • Ischemia of the central nervous system • Tongue claudication • Aortic regurgitation, myocardial infarction • Peripheral neuropathy • Deafness • Tissue gangrene • Common features related to systemic inflammation (40%-100%) • Intense acute-phase response • Anemia (normocytic, normochromic) • Polymyalgia rheumatica • Wasting syndrome
What should the physical examination include? • Careful head and neck examination • Erythema, tenderness, nodularity, thickening of temporal artery, decreased pulse (vs. unaffected temporal artery) • Eye examination • Visual acuity and visual fields • Optic disc and retinal vessels • Assess pulse and blood pressure in all 4 extremities • Listen for bruits over thoracic and abdominal aorta • Listen for aortic regurgitation
What other diagnoses should clinicians consider? • Differential diagnosis of GCA • Common or migraine headache • Atherosclerosis of large vessels • Takayasu arteritis • Headache and temporal artery involvement due to other forms of vasculitis continuted…
Differential diagnosis of Polymyalgia Rheumatica • 30%-50% of patients with GCA also have PMR • Elderly-onset rheumatoid arthritis • Polymyositis/dermatomyositis • Fibromyalgia • Late onset spondyloarthritis • Crystalline arthritis • Cancer-associated muscle pain • Infection-associated muscle pain • Osteoarthritis • Hypothyroidism
What is the role of laboratory testing? • Marked elevations in ESR and CRP: common • Hypochromic or normochromic or normocytic anemia and thrombocytosis: common • Liver function test abnormalities: may be found **No autoantibody tests help identify GCA**
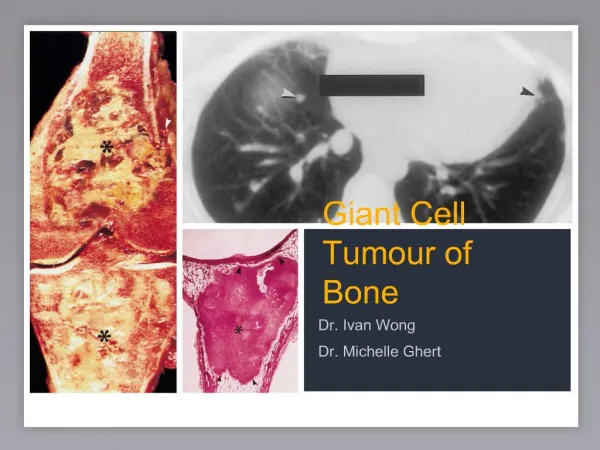
What is the role of temporal artery biopsy in diagnosis? • Characteristic histologic lesions establish diagnosis • Mononuclear cell infiltrates (most in adventitia and media) • Lymphocytes, macrophages, dendritic cells, and giant cells (associated with breakdown of elastic lamina) • Half of biopsies compatible with GCA lack these features • Isolated, periadventitial inflammatory infiltrate or vasculitis of small vessels surrounding temporal artery sometimes only finding on biopsy • To increase diagnostic yield: specimen should be >1 cm long and multiple sections examined
TA biopsy findings in GCA include inflammatory infiltrates consisting of lymphocytes, dendritic cells, macrophages, and multinucleated giant cells
What is the value of imaging studies? • Traditional ultrasound, color duplex ultrasound of temporal artery • Approximately 40-75% sensitivity and 79-83% specificity for diagnosis • MRI • May help identify biopsy-negative GCA patients • Catheter-directed invasive angiography with contrast • Good large and medium vessel resolution, but does not specifically evaluate vessel wall characteristics • FDG-PET • For uncertainty about diagnosis, follow disease activity
When should the clinician consider consulting a rheumatologist or other specialist for diagnosis? • Symptoms atypical • Diagnostic uncertainty exists • Possible large vessel involvement • Help determine need for biopsy • Urgent ophthalmology consultation: for vision loss • Cardiology consultation: aortic murmurs, aortic aneurysms, cardiac ischemia • Surgical consultation: to obtain temporal artery biopsy
CLINICAL BOTTOM LINE: Diagnosis... • Consider GCA in patients older than 50 years with: • New onset, localized unilateral headache • Ischemic symptoms in cervico-cranial and upper extremity vascular territories • Muscle stiffness of the neck, shoulder, pelvic girdle • Physical exam: tenderness, swelling, and erythema over temporal artery; flow abnormalities of large vessels • Lab: ESR or CRP elevated in most patients • Temporal artery biopsy: gold standard for diagnosis
What is the overall approach to treatment? • Don’t delay treating suspected GCA while waiting for a biopsy • High dose oral prednisone • With visual loss: IV pulse corticosteroids • Low-dose aspirin may reduce blindness risk • Methotrexate, other immunosuppressants for repeated flares during tapering • If little improvement within 5 days: revisit diagnosis and consider comorbid conditions causing symptoms
What is the role of steroids in management? • High dose oral corticosteroids • Prednisone or prednisolone 1 mg/kg, up to 60 mg/d • Treat 2 to 4 weeks, followed by slow taper after symptoms and signs of active disease resolve • High dose IV corticosteroids • Methylprednisolone 1000 mg/d for 3 d • For acute vision loss or critical organ ischemia
What are the rationale and role of aspirin? • Controversial whether patients with GCA have increased risks for cardiovascular disease • Studies suggest that low-dose aspirin (≤100 mg/d) diminishes risks of cerebral or ocular and cardiovascular events • Prescribe low dose aspirin to patients who have no contraindications to its use
When should clinicians consider other immunosuppressant medications? • Relapses increase risk of steroid-related complications • Studies have examined immunosuppressives as disease-modifying or steroid-sparing agents • MTX: studies show questionable or modest benefit and MTX associated with potential life-threatening adverse events • Tocilizumab (humanized monoclonal antibody to IL6 receptor): encouraging results for treating relapsing GCA • TNF-a inhibitors: not found to be beneficial for treatment of GCA or reducing steroid requirements
How should clinicians monitor patients being treated for GCA? • Follow initially at 2- to 4-week intervals • Watch for unexplained increases in acute phase reactants, symptom flares with corticosteroid tapering • Ask about cranial symptoms, new onset large vessel ischemic symptoms • Assess blood pressures in both arms and listen for bruits • Order aorta and branch imaging if symptoms of possible new or progressive LVV; consider performing imaging at diagnosis and every 2-5 years • Monitor patients for corticosteroid-related AEs • Ophthalmology follow-up part of routine care
How should clinicians approach immunizations in patients with GCA? • Patients may receive standard vaccinations during periods of stable disease • In absence of proof of established immunity • Avoid live/attenuated vaccines during periods of significant immunosuppression • Make decisions about VZV vaccination and assess concurrent degree of immunosuppression on case-by-case basis • When uncertain, consult an infectious disease specialist
What is the prognosis? • Patients with GCA have normal life expectancy, provided they do not develop complications • MI, stroke, PVD: risk is increased • Aortic dilatation or aneurysms occur in 18%-33% • Aortic reconstruction or intravascular stent placement often required to prevent rupture or dissection • Visual symptoms common • Absence of aggressive treatment within 24 h = very low likelihood of restoring functional vision • Corticosteroid benefits & adverse events have the greatest impact on QOL
How should clinicians educate patients about GCA? • Patients should know to notify physician immediately when they experience symptoms of GCA • Especially symptoms related to organ or regional ischemia • Patients should know about risks and preventive measures for corticosteroid side effects
When should the clinician consider consultation with a rheumatologist or other specialist for treatment? • Rheumatologist • Treatment guidance: relapses, large vessel involvement • Advice: preventing and managing chronic corticosteroid complications • PT, rehabilitation medicine, or counseling • Help coping with GCA, treatment-related side effects • Vascular surgeon • Ischemic symptoms of peripheral or cerebral blood vessels (immediate consultation)
CLINICAL BOTTOM LINE: Treatment... • Start corticosteroids when clinical suspicion high enough to warrant a temporal artery biopsy • Symptoms and acute phase reactants typically respond promptly, but disease flares common • Provide low-dose aspirin to decrease visual and CV ischemic events if no contraindications • Follow patients closely for clinical signs of relapse or LV involvement and for corticosteroid-related complications • Life-long surveillance advised for large vessel involvement