Download

1 / 34
340 likes | 426 Views
Learn about macrolides, a group of antibiotics with a unique lactone ring structure, including erythromycin, clarithromycin, and azithromycin. Explore their mechanism of action, resistance patterns, antibacterial spectrum, and clinical indications.

E N D
Case scenario: A junior doctor prescribed tab. Erythromycin for respiratory infection of a known bronchial asthma patient who was taking theophylline for his asthma. After some days patient experienced nausea, vomiting, tremors and convulsions. What could be the reason for above condition?
MACROLIDES • Means a multimemberedlactone ring structure to which one or more deoxysugar molecules are attached • Prototype is erythromycin • Roxithromycin, clarithromycin & azithromycin are semisynthetic derivatives of erythromycin • Spiramycin is also related but obtained from streptomycesambafaciens Tacrolimus is also a macrolide
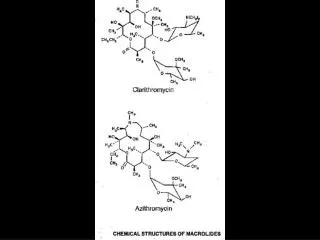
Erythromycin derived in 1952 from strain of Streptomyceserythreus from soil in Philippines • Structure • 14-membered macrocycliclactone ring • Related azalide class has 15-membered ring • FDA approved drugs • erythromycin • clarithromycin • azithromycin • dirithromycin • telithromycin
Protein synthesis inhibitors which act mainly by binding to 50S ribosomal subunits • Macrolides, ketolides, lincosamides, streptogramins, oxazolidinones • Micellaneous drugs include polymyxin-B, colistin (polymyxin-E), mupirocin & fusidic acid
MECHANISM OF ACTION • Binds to the Psite of the 50S bacterial ribosomal subunit. • Aminoacyl translocation and formation of initiation complex are blocked • Inhibitory or BACTERICIDAL
RESISTANCE • Reduced permeability of the cell membrane • Active efflux production (by Enterobacteriaceae) • Esterases that hydrolyze macrolides • Modification of the ribosomal binding site by chromosomal mutation
ANTIBACTERIAL SPECTRUM • Gm +vecocci: strep pneumoniae, strep pyogenes & staphylococci • Gm –vecocci: N gonorrhoeae, M catarrhalis • Gm +ve bacilli: C diphtheriae, B anthracis, L monocytogenes, C tetani • Gm –ve bacilli: L pneumophila, B pertusis, H influenza, H ducreyi
Acid fast bacilli: M kansasii, MA intracellulare, MAC & M leprae • Spirochaetes • M pneumoniae, U urealyticum, C trachomatis
ERYTHROMYCIN • Prototype • Distributed into total body water • Poor CSF penetration • Food interferes with absorption • Serum half life is app. 1.5 h normally and 5 hours in patients with anuria • Not removed by dialysis • Not metabolized and actively secreted in bile ( major route of excretion) • Traverses the placenta and reaches the fetus
Oral- stearate, ethyl succinate, estolate salts • 250-500 mg q 6 h adults, 40 mg/kg/d – children • Parenteral- lactobionate, gluceptate • 0.5-1 g q 6 hours for adults, 20-40 mg/kg/d for children
GIT dysfunction, intrahepaticcholestatic jaundice • Erythromycin metabolites can inhibit cyp p450 enzymes and thus increase the serum concs of theophylline, oral anticoagulants, cyclosporine and methylprednisolone; also oral digoxin by increasing its B/A
Indications for erythromycin 1. Alternative to penicillin in allergic pts ( Staph.Aureus, S. pyogens, S.pneumoniae or T.pallidum ) 2. Diphtheria & whooping cough – drug of choice 3. Legionnaires disease- drug of choice 4. Pneumoniae ( M. pneumoniae ) – children 5. Chlamydia trachomatis
CLARITHROMYCIN • Hydroxylated derivative of erythromycin • more active against Gm (+) pathogens, Legionella and Chlamydia than Erythromycin • lower frequency of GIT effects, less frequent dosing • Longer Half life of 6-7 hours • given at 250-500 mg twice daily
Metabolised in liver to 14-hydroxyclarithromycin • Dose adjustment needed in patients with compromised renal functions • Very effective against • MAC, H influenzae, T gondii, M leprae, H pylori Indications Pharyngitis / tonsilitis Otitis, sinusitis Adjunct in treatment of duodenal ulcer ( H. pylori )
ROXITHROMYCIN • Semisynthetic derivative of erythromycin • Long acting (t1/2 12hrs) • Acid stable, food does not interfere with its oral absorption • More preferred in otitis media, sinusitis, pneumonia c/b M catarrhalis, legionella
AZITHROMYCIN • More active than erythromycin against several gram (-) pathogens • Maintains high concentrations for prolonged periods into a number of tissues (lungs, tonsil, cervix) • Tissue half life – 2-4 days(longest t1/2) • More acid stable with wider tissue distribution
long half-life allows once daily oral administration and shortening of treatment in many cases • a single 1 g dose of azithromycin is as effective as a 7 day course of doxycyclinefor chlamydialcervicitis and urethritis • Community acquired pneumonia – 500 mg loading dose, f/b 250 mg • Does not inactivate cytochrome p450 enzymes and free of the drug interactions that occur with erythromycin and clarithromycin
Indications • Pharyngitis/ tonsilitis ( s. pyogens ), • otitis • sinusitis ( Staph. Aureus & H. influenzae ) • Uncomplicated genital chlamydial infections
SPIRAMYCIN • Oral + I/V • High tissue distribution except CSF • Metabolised in liver & excreted (90%) in the bile • T1/2 is 8hrs • DOC in toxoplasmosis of pregnancy
ADVERSE EFFECTS • Allergic reactions, rashes, fever, eosinophilia, skin eruptions • Cholestatic hepatitis – jaundice, fever, leukopenia • Erythro is associated with reversible ototoxicity • I/V erthromycin is associated with thromboplebitis • Causes diarrhea by stimulating motilin receptors
INTERACTIONS • Erythro & clarithro inhibit CYP3A4 inhibit metabolism & increases the serum levels of theophylline, carbamazepine, statins, warfarin, pimozide, terfenadine & cisapride • Terfenadine, astemizole or cisapride-torsades de pointes(PVT) • Decrease digoxin metabolism by inhibiting microbial flora responsible for degrading digoxin
Macrolides are DOC in (CLAW) • Chancroid • Legionella infections • Atypical pneumonia • Whooping cough
LINCOSAMIDES • Lincomycin (obsolete, not used) & clindamycin • Bind to 50S resulting in bacteriostatic inhibition of bacterial protein synthesis
Streptococci, pneumococci, staphylococci (except MRSA), B fragilis, Clostridium (except difficile) • Excellent against corynebacterium acnes • In combination effective against T gondii & Pneumocystiscarinii
Resistance • Alteration of 50S by adenine methylation • Chromosomal mutation of 50S (receptor alteration) • Drug inactivation by a plasmid mediated adenyltransferase
ADVERSE EFFECTS • Clindamycin associated diarrhoea & PMC • Nausea, vomiting, abdominal cramps & metallic taste • Nm blockade similar to AG • HS reactions
KETOLIDES • Telithromycin & celithromycin • 14 membered ring macrolidesspecificallydesigned for activity against Community acquired RTI • Achieves high tissue concn. in respiratory fluid, saliva, alveolar macrophages & bronchial mucosa • T1/2 - 13.5hrs
Gm +vecocci strep pyogenes, strep pneumoniae, s aureus • Gm –vecocci M catarrhalis, N gonorrhoeae, N menigitidis • Gm –ve bacilli H influenzae, L pneumophila
Telithromycin mainly indicated for macrolide-resistant CAPs, acute exacerbations of chronic bronchitis, sinusitis & streptpharyngitis • Celithromycin more potent than telithromycin
Bacteraemia c/b vancomycin resistant E faecium, skin infections • Nosocomial pneumonia • Combination has a prolonged post-antibiotic effect & hence can be administered at 12hrly, I/V • Pain at the site of infusion & moderate infusion-related arthralgia-myalgia syndrome
REFERENCES • 1. Tripathi K.D., Essentials of Medical Pharmacology 8th ed. Jaypee Brothers 2013 • 2. Satoskar R.S. & Bhandarkar S.D., Pharmacology and Pharmacotherapeutics, 25th ed. Elsevier 2017.