Download
1 / 28
370 likes | 897 Views
Toxoplasmosis. Unit II. Toxoplasma Gondii. Toxoplasmosis is caused by Toxoplasma Gondii which is an obligate intracellular protozoan of worldwide distribution.

E N D
Toxoplasmosis Unit II
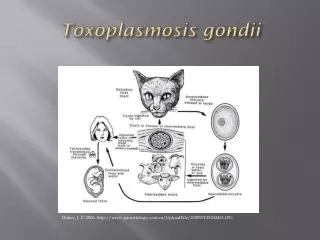
Toxoplasma Gondii • Toxoplasmosis is caused by Toxoplasma Gondii which is an obligate intracellular protozoan of worldwide distribution. • It is acquired primarily orally. Other modes of transmission include the transplacental route , blood product transfusion and organ transplantation. • It can take several different forms: the oocyst; the tachyzoite; and the cyst.
Transmission • Infection can occur by ingestion of oocysts following the handling of contaminated soil or cat litter or the consumption of contaminated water or food sources (such as unwashed garden vegetables). • Transmissionof tachyzoites to the fetus can occur via the placenta following a primary maternal infection. • Transmission can also occur by ingestion of tissue cysts (bradyzoites) present in undercooked meat (especially pork, mutton, and beef) or through transplantation of an organ containing tissue cysts.
Immunocompetent Adults and Children • Toxoplasma gondii primary infection in children and adults (including pregnant women) is asymptomatic in most patients. • In about 10%, it causes a self-limited and non-specific illness that rarely needs treatment. • Very infrequently, myocarditis, polymyositis, pneumonitis, hepatitis, or encephalitis can arise in otherwise healthy individuals.
Ocular Toxoplasmosis • Toxoplasmic chorioretinitis can be seen in the setting of congenital or postnatally acquired disease as a result of acute infection or reactivation. • Clinical manifestations include blurred vision, visual floaters, photophobia and with macular involvement loss of central vision. • Typical findings of toxoplasmicchorioretinitisinclude noticeably white focal lesions with an overlying and intense vitreal inflammatory reaction.
Immunocompromised Patients • These are patients with AIDS, malignancy, on cytotoxic drugs or corticosteroids. • Toxoplasmosis almost always happens as a result of reactivation of chronic infection. • The CNS is the site most typically affected by infection.
Immunocompromised Patients • Clinical manifestations include: • mental status changes • seizures • focal motor deficits • speech disturbances • cranial nerve disturbances • sensory abnormalities • cerebellar signs • movement disorders • neuropsychiatric findings
Immunocompromised Patients • These patients may also present with chorioretinitis, pneumonitis, or multiorgan involvement presenting with acute respiratory failure and haemodynamic abnormalities similar to septic shock.
Congenital Toxoplasmosis • Neonatal clinical manifestations of congenital toxoplasmosis vary widely and include • hydrocephalus • microcephaly • intracranial calcifications • chorioretinitis • strabismus • blindness • epilepsy • psychomotor or mental retardation • petechia due to thrombocytopenia, and anaemia.
Congenitial Toxoplasmosis • The classic triad of chorioretinitis, hydrocephalus, and cerebral calcifications is rather rare. • None of the above mentioned signs is pathognomonic for congenital toxoplasmosis and can be mimicked by congenital infection with other pathogens, including cytomegalovirus, herpes simplex virus, rubella, and syphilis.
Diagnosis • Toxoplasma gondii infection can be diagnosed indirectly with serological methods and directly by PCR, hybridisation, isolation, and histology. • Serologic tests are employed most commonly. • They are sensitive and specific and often are critical in diagnosing acquired and congenital infections.
Diagnosis • Anti-Toxoplasma therapy should be initiated for infants whose initial serologic tests cannot confirm infection, but who have clinical findings consistent with infection. • CSF findings may include elevated protein and variable glucose and WBC counts.
Diagnosis: Neuroradiologic Studies • Computed tomography scan reveals multiple, bilateral, hypodense, contrast- enhancing focal brain lesions in 70-80% of patients. • These lesions tend to involve the basal ganglia and hemispheric corticomedullary junction. • Contrast enhancement often creates a ringlike pattern surrounding the lesion. • MRI is more sensitive than CT scan and thus is the preferred imaging technique.
Differential Diagnosis • CNS Lymphoma • Cryptococcal Meningitis • TBM • CMV Encephalitis
Toxoplasmic Encephalitis • Diagnosis of presumptive toxoplasmic encephalitis based on neuroradiologic studies in patients with AIDS necessitates a prompt therapeutic trial of medications effective against T. gondii. • Clear clinical improvement within 7–14 days and improvement of neuroradiologic findings within 3 wk makes the presumptive diagnosis almost certain.
Primary Prophylaxis • Advise against eating raw meat. • Hands should be washed after touching undercooked meat. • Fruits and vegetables should be washed prior to consumption. • Avoid handling cat litter boxes and gloves should be worn during gardening. • Chemoprophylaxis in patients with CD4 Count < 100/µl
Secondary Prophylaxis • It is given after recovery from Toxoplasmosis Encephalitis and should be given for life. • Some literature states that it can be stopped if patients are free of signs and symptoms and with sustained (> 6 months) increase in CD4 count to > 200/µl on HAART.