Download
1 / 39
390 likes | 530 Views
THE VIOLENT PATIENT Ülkümen Rodoplu ,MD. Overview. Violence in the Emergency Department Recognition of potential for violence Causes of violence in the emergency room Violence Management Physical methods Protocols & Procedures. Psychiatric emergency.

E N D
THE VIOLENT PATIENT ÜlkümenRodoplu,MD
Overview • Violence in the Emergency Department • Recognition of potential for violence • Causes of violence in the emergency room • Violence Management • Physical methods • Protocols & Procedures
Psychiatricemergency • Disturbance in behavior, feelingorthinking • If not attendedto, can result in harmtothepatientorsomeone else. • Duetoexternalorinternalstressoverwhelmingtheperson’sabilitytocope.
Prevalence – Emergency Department • ED often first point of entry • Atmosphere of the ED is oftenone of confusionandrapidplace. • Intoxication, concealed weapons and stress potentially all present at the same time
Why ? • Staff in the ED receive the most amount of verbal and physical abuse out of any other department. • Nature of the work implies exposure to violence. • Methods of violence management are vital
Violence and the Airway • E.P.s predictably encounter both • Final outcome of many pathologies • Failure to manage appropriately leads to injury and/ or death
Recognition of Violence • Aggression • towards an individual • toward creating fear • Stress behaviours in individuals include • use of profanity and verbal outbursts • pacing or frequent alteration of body position or posture • indicate increasing agitation
Causes of Violence • Not always gang related; and not all gang members are violent in certain situations (i.e. child birth) • Understand root of behaviour • psychiatric • drug induced (either intoxication or withdrawal) • child, elder or spousal abuse • frustration due to long waits, unrealistic expectation
Causes of Violence • Overcrowding • Creates volatile situations • Increased waiting times • Neglect of patients who require urgent attention • Proximity of rival groups • gangs • intoxicated driver in close proximity to victims
Incidence • USA • 127 EmergencyDepartment… Result: • Oneverbalthreatdaily (n=41, %32) • Oneweaponthreatdaily(n=23,%18) Lavoie FW, Carter GL, Danzl DF, et al.Emergencydepartmentviolence in United Statesteachinghospitals. AnnEmergMed 1988;17(11):1227-33.
Incidence 5 yearfollowup: • 72 (%57) hospital had theirstaffthretenedwithgun (once). • 55 (%43) hospital had theiremergencystaffthreatenededphysically (once). • 102 (%80) hospital had injury. • 9 (%7) hospital had death. Lavoie FW, Carter GL, Danzl DF, et al.Emergencydepartmentviolence in United Statesteachinghospitals. AnnEmergMed 1988;17(11):1227-33.
Incidence - 2003, StateHospital in Hong Kong - 3 Months 25 caseswith 26 violentpatient … - %64 verbalviolence - None had gun CH Chung. Emergencydepartmentviolence: a localscene. Hong Kong Journal of EmergencyMedicine. Volume 10 Number 1, January 2003
Incidence Reasonsforviolence: • Longwaiting time (%36) • Mentaldisorder(%28) • Dissatisfactionforthecaregiven (%20) • %69 male, 21-50 years of age.. CH Chung. Emergencydepartmentviolence: a localscene. Hong Kong Journal of EmergencyMedicine. Volume 10 Number 1, January 2003
Pathophysiology • Increasedincidence of violenceexists in XYY men. • Increasedtestosterone in manandpremenstrualsyndrome in womenproposed as causes of violentbehavior. • Lowlevels of CSF 5-HIAA found in somewhocommitviolentcrimes • Violentcriminalsdecreasedviolencewithadministration of 2-5-hydroxytryptophan, seratoninprecursor.
Organicreasons • No history of physiatricdisorder • Suddenonsetagitation • Violence → ??? Age 40 ↑
Organicreasons • Intoxication • Hypoglisemia/ Hypoxia • Infection(septisemia, menengitidis) • Organ failure (liver, kidney) • Heatstroke
OrganicReasons • OrganicBrainSyndrome (seizure, trauma, tumor) • Delirium • Trauma • AIDS • Electrolyteabnormality
Pshyciatricdisorders • Schizophrenia • Paranoidideation • Catatonicexcitement • Mania • Bipolaraffectivedisorder
PersonalityDisorders • Borderline • Antisocial • Delusionaldepression • Posttraumaticstressdisorder.
Treatment Modalities • Interview Techniques • Environmental Factors • Physical Restraints • Chemical Control
Case Presentation • 69 yo M, Brought by family after lighting a fire in bathroom.Patient has no complaints.Hx of SchizophreniaP=110, BP 150/90, RR 20, T 37.9No distress, refusing to speak.
What actions are reasonable at this point? • A: One to one observation • B: Undress and fully examine the patient • C: Offer the patient medication • D: Round up sufficient personnel to restrain the patient • E: Stall until you can sign out to your partner before taking any definitive action • F: Medically clear him, transfer to Psych.
Interview Considerations • Calm and Direct • Empathic • Assurance of priorities • Verbalize limits/expectations • Consistency among staff
Interview Techniques • Eye Contact • Personal Space • Door Position • Body Language • Angle of confrontation • Hand and arm position
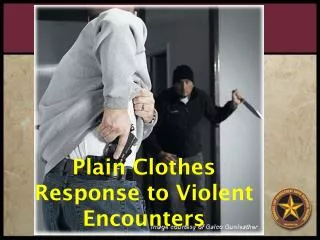
Management throughPhysical Methods • Access control • Minimised unguarded entrances; lock extraneous entrances / exits at night • Secure sensitive areas with access control • Hand-held metal detectors used by security • Enforce visible identification of all staff • Plexiglass between waiting room & ED dept • Block unauthorised vehicle access to the emergency department • Visible security inside & outside
Management throughPhysical Methods • Rankins and Hendey suggest that removing weapons did not decrease number of assaults • Training of ED staff to handle violent situations remains crucial
Management throughProtocol & Procedure • Develop a safety plan with hospital security • Rehearse response mechanisms • Code word called out when violence erupts • Close contact with law enforcement during high-volume or disaster management scenarios • Debrief after major incidents to refine procedures • Access patient history either by records, friends or family to gain proper perspective on a patient • Undress patients to reveal concealed weapons and disarm if necessary
Management throughProtocol & Procedure • Security should recognise an escalating situation • Either between parties or individual misconduct • Separate rival gang members or victim-perpetrator groups • Do not show condescension towards gang members. Cultural differences and language barriers may already cause tension • Immediately use chemical and/or physical restraints with sufficient personnel
Chemical Control • Rapid Tranquilization • Safety • Titratability • Haloperidol • Benzodiazapine • Droperidol
Haloperidol • Buteryphenone antipsychotic • 5- 10 mg. IM, PO, IV • onset 20 minutes • t1/2 of 19 hours • Side Effects
Side Effects • Dystonic Reaction • Akathesia • Neuroleptic Malignant Syndrome • Cardiovascular Effects • Seizure Threshold
Benzodiazapines • Lorazepam • Less predictable effect • Paradoxical disinhibition • Dose requirements • Less titratability • Less Antipsychotic effect • Greater risk of cardiorespiratory depression
Droperidol • Buteryphenone antipsychotic • 2.5- 5 mg IM or IV • Onset minutes • t 1/2 2-4 hours • Side effects
He is still uncooperative. At what point do you decide to physically restrain this patient? • A: Before he does any damage • B: After a psychiatrist has evaluated him and determined a lack of capacity • C: After he does some damage • D: When danger becomes imminent
Physical Restraints • For Imminent Threat of Harm • Preparations • Overwhelming Show of Force • Initiate only When Prepared • Preparation
Physical Restraint • Once Initiated, Swift and Definitive • Suspend Negotiations • Team Leader • Secure Large Joints • Constant Reassurance
What do you do if he tries to leave before you have sufficient personnel? • A: Physically block him • B: Have the nurse physically block him • C: Offer him money to stay • D: Notify local constabulary
Monitoring • Documentation • Neurovascular • Cardiovascular • Airway • Consideration of removal • Transfer Considerations
Summary • Multifactorial approach • Teamwork • Early intervention • Life saving when necessary