Download
1 / 22
270 likes | 612 Views
PARATHYROID HORMONE, HYPERPARATHYROIDISM CKD, & PTH ASSAYS. David Plaut & Shanti Narayanan Summer, 2012. Parathyroid Hormone - PTH. PTH is a hormone secreted by the Parathyroid gland. There are four Parathyroid glands located behind the thyroid. Role of PTH – To Regulate Calcium Levels.

E N D
PARATHYROID HORMONE,HYPERPARATHYROIDISMCKD,&PTH ASSAYS David Plaut & Shanti Narayanan Summer, 2012
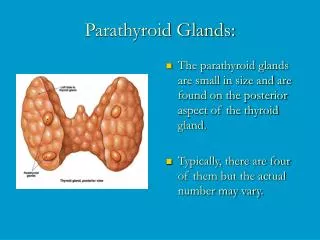
Parathyroid Hormone - PTH • PTH is a hormone secreted by the Parathyroid gland. • There are four Parathyroid glands located behind the thyroid.
Role of PTH – To Regulate Calcium Levels • The Parathyroid glands have only one major function – regulate the calcium level in the body within a very narrow range (8.5 – 10.2 mg/dL) so that the nervous and muscular systems can function properly.
Parathyroid Blood How does PTH regulate Calcium Levels? Increases Calcitriol formation Decreases excretion of Ca Increases excretion of P PTH Calcitriol Ca Calcitriol Bones PTH Store House of Ca & P P PTH Increases Absorption of Ca and P Ca
Causes of Elevated Calcium In 70% of hypercalcaemia (n = 99), the cause was unknown. The second most common diagnosis was skeletal disorders followed by kidney disease. Therefore, PTH analyses should be used more frequently.
Signs and Symptons Roughly three in 10,000 persons are affected by 1o HPT One of the more common causes of hypercalcemia. “Stones, bones, and groans” kidney stones, accelerated bone loss, and GI disomfort. About 15 percent of patients with hypercalcemia have: Weakness. Feeling very tired. Nausea and vomitting Loss of appetite Weight loss for no known reason. Constipation Being much more thirsty than usual Trouble thinking clearly Frequent urination.
Factors Affecting Prognosis and Treatment There are certain issues: ·Whether the calcium level in the blood can be controlled. ·The stage of the cancer. ·Whether the tumor and the capsule around the tumor can be completely removed by surgery. · The patient’s general health.
Treatment of 1o Hyperparathyroidism • Surgery – remove the diseased Parathyroid gland and leave the normal glands. • One bad gland is removed – 95% • 3 or 3 ½ glands are removed – 5%
Secondary Hyperparathyroidism • Secondary implies that the Parathyroid glands grew larger and producing excess PTH in response to kidney disease. • All 4 glands will be enlarged. • Occurs in patients with renal failure. • Occurs in patients who have been on kidney dialysis for several years.
Levels of PTH in CKD – NKF Guidelines • The NKF/K-DOQI Guidelines are derived from studies that used the Allegro Intact PTH assay. NKF / K-DOQI: National Kidney Foundation /Kidney-Dialysis Outcome Quality Initiative
1-84 7-84 1-34 13-34 39-84 53-84 The PTH Molecule • Peptide consisting of 84 Amino acids. • Breaks into small fragments. • Intact PTH is the whole molecule – 1 to 84. 184
Labeled Ab 1-34 39 - 84 1-84 Capture Ab 7-84 1-34 13-34 39-84 53-84 E PTH Assay Design
PTH Assays • 1st Gen Assays: Not Specific for Intact PTH. • High cross reaction with PTH fragments. • 2nd Gen Assays: Used different epitopes for the N-terminal and C-terminal fragments. • 3rd Gen Assays: Not commercialized. • Significant variation in assay results between different manufacturers. • Use of different epitopes for antibody binding • Lack of standardization.
Intra-operative PTH: Cost Benefit Analysis • Conventional Surgery without using Intra-operative PTH • Standard operation using Intra-operative PTH • MIRP using Intra-operative PTH • Surgery cost : ~ $ 4500. • Frozen sections: • ~ $ 1000. • Hospital stay: ~ $ 3200. • Total cost: ~ $ 8700. • Surgery cost : ~ $ 3200. • Frozen sections: $ 0. • PTH assay: ~ $ 100. • Hospital stay: ~ $ 3200. • Total cost: ~ $ 6500. • Surgery cost : ~ $ 3200. • Frozen sections: $ 0. • PTH assay: ~ $ 100. • Hospital stay: $ 0. • Total cost: ~ $ 3300. SAVE $5400 SAVE $2200
PTH Assays and Parathyroidectomy Intraoperative PTH measurement with a decrease of at least 90% in intra-operative PTH is highly predictive of successful parathyroidectomy and normalization of postoperative calcium and PTH levels.
How Many Samples Are Needed? The study found that an intra- operative PTH determination with a > 50% change is an excellent prognostic marker of resolution and that only 2 samples are required: one at baseline another 10 min. after removal of the abnormal tissue.
PTH in Renal Patients Intraoperative decay of PTH during operation for renal HPT is somewhat slower in patients with renal HPT than for patients with normal renal function. 20 min after resection, a decline to < 50% of the pre-operative level predicts cure, while <40% predicts a failure to cure.
Calcium Assays with PTH Assays? The mean baseline PTH level dropped by 70% at 5 minutes after removal of the abnormal glands and by 83% at 10 minutes. The mean baselines of both TSC and ICa dropped by 4% at 5 minutes after removal of the abnormal glands and remained at 4% at 10 minutes. Decreases in TSC and ICa during parathyroidectomy are minimal. Unlike PTH levels, TSC and ICa levels do not consistently decrease at 5 and 10 minutes after gland resection.
Calcium Levels and Parathyroidism Doubling the number of serum calcium analyses did not increase the detected number of raised calcium levels. More frequent PTH analyses resulted in a corresponding increase in detected high PTH levels. 15% of the patients with hypercalcaemia were diagnosed with primary hyperparathyroidism. Over 40% of patients with primary hyperparathyroidism in the study had only slightly raised serum calcium levels.
PTH Assays vs. Other Tools. The positive predictive values: sestamibi scanning 81% radioguided surgery 88% PTH 99.5% Perioperative PTH testing has the highest sensitivity, positive predictive value, and accuracy. The inherent variability of sestamibi scanning and radioguided techniques emphasizes the critical role of PTH testing during parathyroid surgery.
Questions ?Comments Thank you avi
THANK YOU • Davidplaut@yahoo.com