Download
1 / 39
420 likes | 1.24k Views
Megan Keiser, RN, DNP(c), CNRN, APRN MANS/AANN-SEM Chapter Meeting June 2011. What is Stroke?. Objectives. Define “stroke.†Explain the historical perspective of stroke. Describe the epidemiology of stroke. List the different types of stroke. List the different causes of stroke.

E N D
Megan Keiser, RN, DNP(c), CNRN, APRN MANS/AANN-SEM Chapter Meeting June 2011 What is Stroke?
Objectives • Define “stroke.” • Explain the historical perspective of stroke. • Describe the epidemiology of stroke. • List the different types of stroke. • List the different causes of stroke.
Disclosures • Elected officer (Secretary/Treasurer) of the American Association of Neuroscience Nurses (AANN). • Neurosurgery Nurse Practitioner at William Beaumont Hospital, Royal Oak, MI • No financial conflicts of interest.
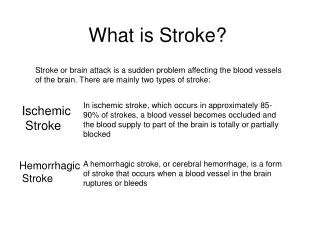
Stroke • A stroke is the sudden death of a portion of the brain cells due to a lack of oxygen. • The World Health Organization (1980) defines stroke as “rapidly developing clinical signs of focal (at times global) disturbance of cerebral function, lasting more than 24 hours or leading to death with no apparent cause other than that of vascular origin.”
History of Stroke • Hippocrates, the father of medicine, first recognized stroke over 2,400 years ago. • At this time stroke was called apoplexy, which means "struck down by violence" in Greek. • This was due to the fact that a person developed sudden paralysis and change in well-being. • Physicians had little knowledge of the anatomy and function of the brain, the cause of stroke, or how to treat it.
History of Stroke • It was not until the mid-1600’s that Johann Jacob Wepfer found that patients who died with apoplexy had bleeding in the brain. • He also discovered that a blockage in one of the brain's blood vessels could cause apoplexy.
History of Stroke • Medical science continued to study the cause, symptoms, and treatment of apoplexy and, finally, in 1928, apoplexy was divided into categories based on the cause of the blood vessel problem. • This led to the terms stroke or "cerebral vascular accident (CVA)."
History of Stroke • Stroke is now often referred to as a "brain attack" to denote the fact that it is caused by a lack of blood supply to the brain, very much like a heart attack is caused by a lack of blood supply to the heart. • The term brain attack also conveys a more urgent call for immediate action and emergency treatment by the general public.
Why is it called a “stroke?” • "Stroke" is a literal translation of the original Greek term "apoplexy". • “The explanation, for centuries, was that someone had been struck down by God.” • Because many people woke up in the morning with symptoms, it was said to occur at the “stroke of midnight” and, thus, it was called a stroke.
Epidemiology of Stroke • Prevalence • Among adults age 20 and older, the estimated prevalence of stroke in 2006 was 6,400,000. • About 2,500,000 males and 3,900,000 females. • Incidence • Each year about 795,000 people experience a new or recurrent stroke. • About 610,000 of these are first attacks, and 185,000 are recurrent attacks.
Epidemiology of Stroke • Incidence • On average, every 40 seconds someone in the United States has a stroke. • Each year, about 55,000 more women than men have a stroke. • Men’s stroke incidence rates are greater than women’s at younger ages but not at older ages. • The male/female incidence ratio is 1.25 at ages 55–64; 1.50 for ages 65–74; 1.07 at 75–84 and 0.76 at 85 and older. • Blacks have almost twice the risk of first-ever stroke compared with whites. • The age-adjusted stroke incidence rates at ages 45–84 are 6.6 per 1,000 population in black males, 3.6 in white males, 4.9 in black females and 2.3 in white females
Epidemiology of Stroke • Mortality • Stroke accounted for about one of every 18 deaths in the United States in 2006. • Stroke mortality for 2006 was 137,119 (54,524 males, 82,595 females). • When considered separately from other cardiovascular diseases, stroke ranks No. 3 among all causes of death, behind diseases of the heart and cancer. • On average, every four minutes someone dies of a stroke. • Among people ages 45–64, 8 to 12 percent of ischemic strokes and 37 to 38 percent of hemorrhagic strokes result in death within 30 days.
Epidemiology of Stroke • Mortality • From 1996–2006, the stroke death rate fell 33.5 percent and the actual number of stroke deaths declined 18.4 percent. • The 2006 final death rate for stroke was 43.6 per 100,000. • Death rates were 41.7 for white males and 67.1 for black males; 41.1 for white females and 57.0 for black females. • Because women live longer than men and stroke occurs at older ages, more women than men die of stroke each year. Women accounted for 60.6 percent of U.S. stroke deaths in 2006.
Epidemiology of Stroke • Aftermath • Stroke is a leading cause of serious, long-term disability in the United States. • The median survival time (in years) following a first stroke is: • at ages 60–69: 6.8 for men and 7.4 for women. • at ages 70–79: 5.4 for men and 6.4 for women. • at age 80 and older: 1.8 for men and 3.1 for women. • After stroke, women have greater disability than men. In an analysis of 108 stroke survivors from the Framingham Heart Study, 34 percent of women were disabled six months after their stroke compared to 16 percent of men.
Epidemiology of Stroke • Cost • The estimated direct and indirect cost of stroke for 2010 is $73.7 billion. • The mean lifetime cost of ischemic stroke in the United States is estimated at $140,048. • This includes inpatient care, rehabilitation and follow-up care necessary for lasting deficits.
The “Stroke-Belt” • The stroke belt was first identified in 1962 by Centers for Disease Control (CDC) researchers who noted a concentration of high stroke death rates in the Atlantic coastal plain counties of North Carolina, South Carolina and Georgia.[4] Similar high stroke rates were later observed in the Mississippi Delta region as well.
The “Stroke-Belt” • Analysis by the CDC of U.S. mortality statistics from the period 1991 to 1998 found that for both blacks and whites the counties with the highest stroke death rates were in the southeastern states and the Mississippi Delta region. • The causes of the elevated incidence of stroke in the stroke belt region have not been determined. • Numerous possible contributing factors have been identified, including race, hypertension, low socioeconomic status, diet, quality of healthcare facilities, smoking, and infections.
Non-modifiable Age (> 55) Gender (male>female) Heredity Race (>Hispanic, Asian, African American) Prior stroke, TIA, MI Modifiable HTN Smoking Obesity High-fat Diet High cholesterol Diabetes Genetic disorders A-fib Carotid artery disease Risk Factors for Stroke
What is an ischemic stroke? • A thromboembolic stroke occurs when one of the blood vessels in the brain is blocked so that an area of the brain has restricted or absent blood flow for a period of time long enough to cause permanent damage.
What causes an ischemic stroke? • Thrombus: a blood clot that obstructs flow to a blood vessel • Embolus: something that travels through the bloodstream, lodges in a blood vessel and blocks it – this usually refers to a piece of fat or atherosclerotic plaque when discussing stroke • Surgical retraction • Vessel sacrifice
Signs and symptoms? • Hemiparesis or hemiplegia • Numbness • Decrease or loss of vision • Speech difficulty • Swallowing difficulty • Headache • Vertigo or dizziness • Loss of coordination • Decreased level of consciousness
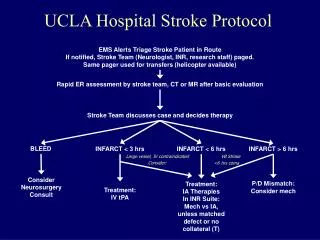
Treatment for ischemic stroke: • TIME IS BRAIN!!!! • Intravenous tPA • Intra-arterial tPA • Clot retrieval • When is it surgical???
Intravenous tPA • Thrombolytics restore cerebral blood flow in some patients with acute ischemic stroke and may lead to improvement or resolution of neurologic deficits • Symptom onset clearly documented within 3-4.5 hours of tPA infusion • Know the exclusion criteria
Intra-arterial tPA • IA tPA is a faster way to deliver clot-busters directly to the blockage. • Requires a cerebral arteriogram • Expands the window of treatment to 6 hours
Clot Retrieval • Mechanical clot retrieval device = MERCI • Opens the window to 8 hours after symptom onset • Requires cerebral arteriogram • “Corkscrew” device is forced into thrombus and removed • Causes recanalization of blood vessel and restoration of blood flow
When is it surgical??? • Topic of much debate • Younger patients with non-dominant hemisphere CVA and intractable intracerebral edema may be offered a decompressive craniectomy
What is a hemorrhagic stroke? • Hemorrhagic stroke occurs when a blood vessel bursts inside the brain. The brain is very sensitive to bleeding and damage can occur very rapidly, either because of the blood itself, or because the blood increases pressure in the brain.
What causes a hemorrhagic stroke? • High blood pressure is leading cause • Conversion of thrombotic stroke (tPA) • Aneurysm or AVM rupture • Amyloid angiopathy • Hemorrhages in or around brain tumors • Anticoagulation • Clotting Disorders
Aneurysm Rupture • An aneurysm is a ballooning out of a blood vessel which makes it weak and prone to hemorrhage
AVM Rupture • AVMs are an abnormal area of blood vessels that have many weak spots prone to hemorrhage. Cavernomas are a type of AVM in which the vessels are very small, but they are still prone to hemorrhage.
Amyloid Angiopathy • Accumulation of protein called amyloid within artery walls, particularly in the elderly.
Hemorrhages in or around brain tumors • Either as a result of surgery or because the tumor is eroding through blood vessels.
Treatment for hemorrhagic stroke: • FIX WHATEVER CAUSED IT!!! • Control blood pressure • Clip or coil the aneurysm • Resect/embolize the AVM • Reverse anticoagulation • Give platelets if necessary • When is it surgical???
When is it surgical??? • Topic of much debate • Early treatment of ruptured aneurysm – later for ruptured AVM • Almost never to evacuate the clot – too deep! • Exception – cerebellar IPH • Decompressive craniectomy
Cerebellar IPH • Infratentorial vs. supratentorial • Decompressive suboccipital craniotomy and evacuation of clot
Clot catheters & intraclot tPA • Used for spontaneous IPH • Sometimes used in conjunction with EVD if clot has ruptured into the ventricle
Nursing implications: • Know your stuff when it comes to tPA • Know when you’re getting into trouble – worsening or new deficits are a red flag! • Know what questions will be asked when you call a physician • Aggressive BP management is crucial • Prevent complications • Early rehab is a nursing function
Questions • MKeiserRN@aol.com or mkeiser@beaumonthospitals.com