Download
1 / 39
400 likes | 1.52k Views
Biliary anatomy. Common variants:TrifurcationRight anterior or posterior hepatic duct branches from common duct Cystic duct is variable in its course, may join right hepatic duct. Biliary anatomy. Biliary anatomy. Cystic artery is usually a branch of the R hepatic. Biliary histology. Layers of gallbladder:Epithelium (columnar)Lamina propriaSmooth muscleSubserosal connective tissueSerosaNo submucosa or muscularis mucosa!.

E N D
1. Benign biliary disease and biliary injury- biliary physiology, pathology, presentation and management Claire Edwards
09/09/09
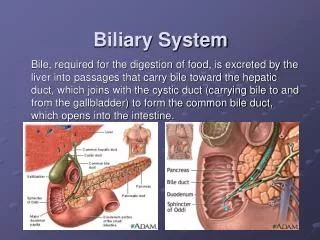
3. Biliary anatomy
4. Biliary anatomy Cystic artery is usually a branch of the R hepatic
5. Biliary histology Layers of gallbladder:
Epithelium (columnar)
Lamina propria
Smooth muscle
Subserosal connective tissue
Serosa
No submucosa or muscularis mucosa! CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi
CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi
6. Biliary physiology Liver produces 0.5 to 1.0 L bile/day
Vagal input, GI hormones (cholecystokinin, secretin, gastrin) increase bile production
GB epithelium absorbs sodium and water, secretes mucin and acid.
CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi. Bile in GB is concentrated relative to bile from liver. Active sodium transport, passive water absorption
CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi. Bile in GB is concentrated relative to bile from liver. Active sodium transport, passive water absorption
7. Biliary physiology Contents of bile: water, electrolytes, bile salts, proteins, lipids, bile pigments
Primary bile salts: cholate, chenodeoxycholate
Conjugated w/ glycine, taurine in liver to become bile acids
95% of bile acids are re-absorbed via enterohepatic circulation
Cholesterol crystals, mucin are nucleating agents for stones.
Decreased stability of cholesterol-containing vesicles
8. Jaundice �Conjugated (direct) bili? increased in biliary obstruction
Unconjugated (indirect) bili? increased in hemolysis, hepatocellar injury
Scleral icterus at >2.5 mg/dL
Jaundice at > 5 mg/dL
9. Gallstones �Of those with gallstones, 1% per year develop serious symptoms or complications and need cholecystectomy.
Risk factors: Crohn�s disease, terminal ileal resection, TPN/fasting
States of excess cholesterol contribute to cholesterol gallstones
10. Gallstones �Pigment stones
Dark 2/2 calcium bilirubinate
Black pigment stones: hemolytic states, cirrhosis
Brown pigment stones
Within bile ducts
Associated with infection, biliary stasis
11. Gallstones �Biliary colic
Only assoc. w/ meals in 50%
Pain attack lasting > 24 hrs? acute rather than chronic cholecystitis
Biliary colic, no stones, sludge detected on more than one occasion ? lap chole
Biliary symptoms may also be caused by cholesterolosis, polyps (see later)
12. Cholecystitis �Presentation: N & V, pain, fever, persistent (unlike colic) RUQ or epigastric pain,
Acute cholecystitis�exacerbated by touch: Murphy�s sign is due to peritoneal irritation.
Most cases? gallstone dislodges, inflammation resolves
Or may lead to inflammation and necrosis of the GB wall (gangrenous cholecystitis)? GB abscess
Secondary infection w/ gas forming organisms? emphysematous cholecystitis
13. Acute Cholecystitis Management: early cholecystectomy (2-3 days)
Morbidity, length of stay, return to work all better w/ laparoscopic chole
Predictors of conversion to open: older age, higher ASA, male gender, thickened GB wall, obesity
GB empyema, perforation, emphysematous cholecystitis? need emergency cholecystectomy
If cannot see to ligate cystic duct 2/2 inflammation? partial cholecystectomy, cauterization of remaining GB mucosa, drainage
OR if pt too unstable for OR? cholecystostomy tube, IV abx, then lap chole in 3 months
14. Choledocholithiasis Primary stones: biliary stasis (stricture, papillary stenosis, tumors, secondary stones), biliary infection
Secondary calculi: started in GB, then migrated.
�Retained� if discovered < 2 years after cholecystectomy (1-2%)
�Recurrent� if discovered > 2 yrs after cholecystectomy
Dx: consider MRCP; ERCP is potentially therapeutic as well as diagnostic
Complete endoscopic clearance of common duct stones: 75% of pts w/ one procedure, 90% w/ multiple procedures.
15. Imaging Ultrasound:
>98% sensitive, > 95% specific for stones
Cholecystitis: ductal dilation, pericholecystic fluid, wall thickening, sonographic Murphy�s sign
Common bile duct? upper limit of nl is 7 mm
Extrahepatic ducts > 10 mm or intrahepatic ducts > 4 mm suggests obstruction
GB wall is thickened if > 4 mm.
Mass lesion evidence: stone that does not move when patient does, asymmetric thickening
16. Imaging KUB shows 15% of stones (only show up if calcified)
CT
Cholangiography: Noninvasive. IV contrast, excreted in biliary system. Good for ductal anatomy.
Only about 60% sensitive for stones (only show up if calcified)
MRC: Good for common bile duct stones
PTC: Used instead of ERCP for proximal stones.
17. Imaging HIDA:
Cystic duct obstruction is present if GB not visualized 2 hours after injection
Biliary dyskinesia: Ejection fraction less than 35% at 20 minutes after CCK administration is considered abnormal.
Nl HIDA excludes acute cholecystitis.
High false positive rate when pt is fasting (passage of tracer slows)
18. Normal HIDA scan
19. Abnormal HIDA scan
20. Other indications for cholecystectomy Gallstone pancreatitis
Remove GB same admission
Biliary dyskinesia
21. Lap chole Conversion rate should be 5%. In acute cholecystitis may be up to 30%.
2nd trimester in pregnant women
CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi
CCK: released from duodenum when intraluminal fat, amino acids, and gastric acid are present; also causes relaxation of the Sphincter of Oddi
22. Laparoscopic cholecystectomy: critical view
23. Postcholecystectomy pain With jaundice, biloma, or significant pain? ERCP looking for retained stone or CBD injury or stricture
24. Complications of cholecystectomy Bile duct injury
25% are recognized intraoperatively
Primary repair over T-tube if small, nonthermal injury
Otherwise, choledochojejunostomy
If recognized post-op AND in the presence of leak, wait 6 weeks (too much inflammation)
Biliary stricture
If returning to OR, success is increased by getting a percutaneous or ERCP cholangiogram preop
Biliary-enteric bypass more successful than primary end-to-end biliary repair
Ischemic biliary strictures will not respond permanently to IR/endoscopic dilation Remember drains, referral to tertiary center is an option
Remember drains, referral to tertiary center is an option
25. Complications of cholecystectomy Biliary leak
From cystic duct stump (acute cholecystitis inflammation can make clips come off) or duct of Luschka
Widely drain and do endoscopic stenting, too much inflammation in presence of bile leak to re-repair
26. Complications of cholecystectomy Bismuth classification of biliary injuries:
Type I: > 2 cm below hepatic duct bifurcation
Type 2: < 2 cm
Type 3: hepatic duct confluence is intact but no residual common hepatic duct exists
Type 4: destruction of hilar confluence, L and R hepatic ducts are completely separated
Type 5: involve branch of right hepatic duct +/- the common bile duct Bismuth classification determines whether you will have to do individual hepaticojejunostomies of the left and right ducts
Bismuth classification determines whether you will have to do individual hepaticojejunostomies of the left and right ducts
27. Gallstone ileus �Tumbling obstruction�
Terminal ileum? most common site of obstruction due to narrow lumen
Enterotomy, milk stone proximally and out
Make sure bowel does not need to be resected in the area where the stone was impacted
Closure of biliary-enteric fistula and cholecystectomy (at second laparotomy if there is too much RUQ inflammation)
28. CBD exploration Perform choledochotomy
Leave 16 Fr or larger T-tube in place.
Follow-up cholangiogram
Clamp tube and pull in 4-6 weeks if no more stones
If stones still present, removal via T tube in 4-6 weeks
Or transduodenal sphincterotomy (if stone impacted at ampulla)
Lap CBD exploration:
Transcystic approach vs. choledochotomy approach
saline irrigation, stone basket or choledochoscope via cystic duct
Larger stones need choledochotomy approach. CBD needs to be at least 6 mm
Need T-tube
Need drainage procedure when stones cannot be cleared or duct is > 1.5 cm in diameter.
Sphincterotomy: incise sphincter at 11:00 position to avoid pancreatic duct.
Drainage procedure: choledochoduodenostomy or choledochojejunostomy, depending on ability to mobilize the duodenum and tension on the anastomosis. Duodenal anastomosis can result in sump syndrome (obstruction by food) Sphincterotomy: incise sphincter at 11:00 position to avoid pancreatic duct.
Drainage procedure: choledochoduodenostomy or choledochojejunostomy, depending on ability to mobilize the duodenum and tension on the anastomosis. Duodenal anastomosis can result in sump syndrome (obstruction by food)
29. Acute acalculous cholecystitis More fulminant course than calculous cholecystitis
Possibly related to visceral ischemia, gallbladder stasis
Risk factors: elderly, TPN, major abdominal surgery (AAA)
U/S is test of choice. HIDA has high false (+) rate.
Percutaneous cholecystostomy in those who cannot go to OR (90% improve)
30. Acute cholangitis Have to have obstruction (usu. common duct stone)
Must do cholangiography
If very sick/septic needs urgent biliary decompression/relief of obstruction? PTC or ERCP
31. Recurrent pyogenic cholangitis Intrahepatic stones from infection w/ biliary bacteria or parasites (Clonorchis sinensis, Opisthoricis, Ascaris)
Asian population
Recurrent episodes of cholangitis due to partial obstruction
Possibly hepatic abscesses, cirrhosis
Risk for cholangiocarcinoma
Roux-en-Y hepaticojejunostomy w/subcutaneous afferent (Hudson) loop for endoscopic access
Extended hepatectomy of dominant stone-containing lobe, if there is one, for cholangiocarcinoma risk
32. Primary sclerosing cholangitis Intra- and extrahepatic biliary strictures
60-70% have ulcerative colitis
1% per year risk of cholangiocarcinoma
Endoscopic/percutaneous brushings of strictures for surveillance
Jaundice, pruritis, fatigue
10-12 years average lifespan from time of diagnosis
DX: cholangiography
If end-stage liver disease? transplant.
85% 5 year survival
Medical therapy: �disappointing,� ursodeoxycholate only improves numbers, not patient Rapid onset of jaundice, CA 19-9 > 100 are helpful but not predictive in cholangiocarcinoma
Rapid onset of jaundice, CA 19-9 > 100 are helpful but not predictive in cholangiocarcinoma
33. Benign biliary strictures Multiple causes: pancreatitis, cholangitis, etc.
Anastomotic strictures: Have to do PTC to dilate biliary-enteric anastomosis because difficult to access Roux en Y endoscopically.
34. Choledochal cysts Anomalous biliary duct-pancreatic duct junction with long common channel, reflux of pancreatic enzymes, and cystic breakdown of biliary tract
10 % have classic triad of RUQ pain, jaundice, palpable mass
Severe possible complications: cirrhosis, portal hypertension, cyst rupture w/ bile peritonitis
GB, liver, or cholangiocarcinoma incidence? 3 to 25%
U/S, CT scan to diagnose; cholangiography to plan operative treatment
35. Choledochal cysts Type I: Extrahepatic
Type II: diverticular extrahepatic
Therapy for Type I and II cysts: cholecystectomy, resection of extrahepatic bile ducts w/ hepaticojejunostomy
TypeIII: Intraduodenal
Type IVa: extrahepatic and intrahepatic
Type IV b: multiple sections of extrahepatic bile ducts
Tx: resect extrahepatic cyst
Type V: Caroli�s disease. Intrahepatic ducts only.
Do liver resection of involved area if possible.
Liver transplantation
Type I: Extrahepatic
Type II: diverticular extrahepatic
Therapy for Type I and II cysts: cholecystectomy, resection of extrahepatic bile ducts w/ hepaticojejunostomy
TypeIII: Intraduodenal
Type IVa: extrahepatic and intrahepatic
Type IV b: multiple sections of extrahepatic bile ducts
Tx: resect extrahepatic cyst
Type V: Caroli�s disease. Intrahepatic ducts only.
Do liver resection of involved area if possible.
Liver transplantation
36. Biliary fistulas Cholecystoenteric fistula
From gallstone eroding into viscus:
#1 duodenal, #2 colon
Mirizzi�s syndrome: Stone impacted in neck of GB or in cystic duct? inflammation? hepatic duct obstruction? jaundice
From PUD: choledochoduodenal or choledochogastric fistula
Rarely, from malignancy or trauma
37. Polypoid lesions of the gallbladder Cholesterolosis: deposits of cholesterol in GB wall
Cholesterol polyp: pedunculated, epithelialized focus of cholesterolosis
No shadow on U/S
Adenomatous hyperplasia: increased thickness of mucosa and muscle
Mass lesion on U/S
Adenomatous polyp: true neoplasm
Granular cell myoblastoma: benign tumor of neuroectoderm, needs cholecystectomy Symptomatic? cholecystectomy
Suspicion of carcinoma (e.g., invasion by U/S)? open cholecystectomy
Otherwise if less than 1 cm, observe.
Fibroxanthogranulomatous inflammation: Foamy histiocytes/inflammatory cells/fibroblastic vascular rxn/mucosal ulcerationSymptomatic? cholecystectomy
Suspicion of carcinoma (e.g., invasion by U/S)? open cholecystectomy
Otherwise if less than 1 cm, observe.
Fibroxanthogranulomatous inflammation: Foamy histiocytes/inflammatory cells/fibroblastic vascular rxn/mucosal ulceration
38. Benign biliary lesions Papilloma or adenoma of bile duct
Often jaundice b/c often close to ampulla
Resect lesion w/ some duct wall (to avoid recurrence)
Transduodenally for ampullary lesions
Benign inflammatory tumors: pseudotumors
Usually extrahepatic, but above biliary bifurcation.
39. References Townsend, C.M., ed. 2008. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 18th ed. Philadelphia: Saunders Elsevier.
Mulholland, M., ed. 2006. Greenfield�s Surgery: Scientific Principles and Practice, 4th ed. Philadelphia: Lippincott Williams and Wilkins.
HIDA scan images downloaded from �Emedicine: Cholecystitis: Multimedia.� http://emedicine.medscape.com/article/171886-media
Bines, S.D., et.al. 2007. Rush University Medical Center Review of Surgery. Philadelphia: Saunders Elsevier.