Download
1 / 103
1.06k likes | 1.31k Views
ARTHROGRAMS RT 255. Radiography of a joint space or it’s surrounding structures with injection of contrast media. ARTHROGRAMS. Injected into JOINT SPACES “DOUBLE CONTRAST” IODINE (positive contrast) WATER soluble (Ionic or Non-Ionic) AIR (negaitve contrast).

E N D
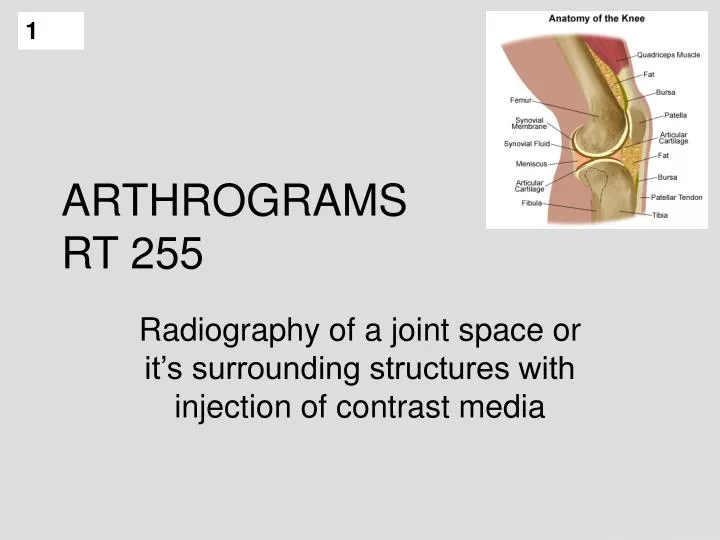
ARTHROGRAMSRT 255 Radiography of a joint space or it’s surrounding structures with injection of contrast media
ARTHROGRAMS • Injected into JOINT SPACES “DOUBLE CONTRAST” • IODINE (positive contrast) • WATER soluble • (Ionic or Non-Ionic) • AIR (negaitve contrast)
Arthrography is concerned with synovial joints MOSTLY REPLACED BY MRI – non invasive, good detail of soft tissue structures CONTRAINDICATIONS TO MRI: • CLAUSTROPHOBIC • PT SIZE • Foreign Body (metal) • COST / INSURANCE REIMBURSEMENT
Anatomy of a Synovial Joint • Synovial membrane • Menisci, fat pads, and intra-articular disks • Ligaments
INDICATIONS FOR EXAM • This procedure is used to obtain diagnostic information regarding the joints and surrounding soft tissues or cartilage. • ligament, meniscus (cartilage), bursa Usually done for the knee • shoulder, hip, wrist, TMJ
Indications and Contraindications for Arthrography • Indications: • Suspected injury of meniscus (tears) • Suspected capsular damage • Rupture of articular ligaments • Cartilaginous defects • Arthritic deformities (specifically TMJ) • Congenital luxation ( dislocation) of hip • Extent of damage from trauma • Contraindications: • Hypersensitivity to iodine
Clinical Symptoms • Pain • Swelling • Limited range of motion • Recurrent instability (such as ankle)
Contrast media • Contrast INJECTED into joint space – capsular space – bursa (30 – 100 ml may be needed) • CONTRAST – water based only – iodinated (ionic or nonionic) • Negative , positive or both (Double Contrast) • Negative – room air, CO2 • Possible hazard of air is an air embolism • Water-soluble contrast agents – easily absorbed
Contrast Mediakeep bottle in room until end of studyhave several syringes available
PROCEDURE – PREP • Patient Prep – (none prior to exam) • Pt comfort (gown, empty bladder) • get history • check allergies • SKIN PREP – may need to shave area of injection • betadine scrub – circular motions
Sterile Procedure GLOVES GOWN (?)
Sterile tray “arthrogram tray” Aseptic technique for skin cleansing • (betadine – check for allergy) • Local anesthetic • (usually on tray, put may have to draw up – sterile procedure) • do not contaminate tray
Aseptic Technique betadine scrub
SUPPLIES Needles used – • length and gauge depends on part being examined • DR may aspirate joint prior to injection of contrast media • (have large syringes available) • Sterile gauze, towels, ace bandages
Needles • Smaller gauge has a larger number • Larger gauge has a smaller number • Length and gauge of needle is usually part of protocol • DR’s preference • Part being examined
Aspiration • Dr’s may aspirate fluids before injecting contrast media • If there is a joint effusion especially • Fluid is sent to lab in specimen vials
KNEE ARTHOGRAM Most common problem : • Pain and Swelling, • Limited ROM (range of motion) • athletic injuries • Knee support to stress knee • Contrast Injected – then part is stressed or moved to work contrast into joint spaces –
RADIOGRAPHY • SCOUT FILMS • AP • LATERAL • Other • (CHECK WITH Radiologist)
KNEE ARTHROGRAM(MOST COMMON) Air and contrast material injected into the joint reveal the outlines of the joint space including the supra patellar pouch
FILMING - KNEE Filming done under fluoroscopy (Knee spot films may be done 9 on 1) Knee stressed to see medial and lateral meniscus • DOUBLE CONTRAST KNEE – FILMS TAKEN WITH HORIZONTAL BEAM = • contrast moves down – air moves up – shows good delineation of tissues
For Cruciate ligamentspatient may sit on end of table with knee flexed 90 degrees – • Then a cross table lateral taken
Knee Arthrogram • Place PT prone • Place PT in frame or stress device to open JT space • Sometimes support is placed under distal femur and small sandbag on ankle to widen JT space • Part is manipulated to disperse contrast and often multiple spot films are taken under fluoroscopy
Knee Arthrogram • Overheads are done • AP, lateral, 20 degree right and left oblique • Sometimes Interconyloid fossa projections are required • Single contrast study for a torn meniscus may fail to demonstrate the tear • Usually single contrast studies are used to demonstrate loose particles of the JT • Post procedure • PT may feel tightness • This should go away in 1-2 days • Can be treated with analgesics
Meniscus Tears • Symptoms may include: • "Popping" sound at the time of the injury • Pain • Tightness • Swelling within the knee, often called "water on the knee" • Locking up, catching, or giving way of the knee • Tenderness in the joint
Knee Arthrogramdouble contrast study • smaller amounts of contrast can be used • Decreases discomfort to PT • Provides are more accurate study • Demonstrates menisci the best • Positive contrast coats menisci • Air rises
Knee Arthrogram: • Apply same principles Scout films: often AP, Lateral and oblique • Check with DEPT protocol • Anesthetic injected • Contrast is injected (double contrast study) • PT placed semiprone • Knee is manually stressed while spot films are taken (medial & lateral meniscus)
Horizontal Knee Radiographs Spot Films Medial Meniscus AP LAT
For Cruciate Ligaments • Double Contrast study • PT’ s sits with knee flexed 90 degrees over the side of the table • Firm pillow placed under knee so that forward pressure can be applied • PT holds IR with grid • Closely collimate • Tightly overexposed lateral projection is made
CT Knee Arthrography • PT gets a regular arthrogram in radiology • Then is taken to CT for imaging • Can be single or double contrast (water soluble iodine) • Usually double
MRI Knee Arthrography • Gadolinium contrast is used • Contraindications include metal in body, claustrophobia, & PT size