Download

1 / 77
770 likes | 1.07k Views
SGD 2: RHD. Saldana Emmanuel, Sales Stephanie, Salonga Cryscel, San Diego Phoebe, San Pedro Rina , Sanez Eric, Sanidad Erica, Santos Emmalene , Santos Jeniffer , Santos Joel, Santos Karen,Santos Mary Elaine. Elvie, 28 y/o housewife, dyspnea. 3 days PTA. Dental Procedure. 2 days PTA.

E N D
SGD 2: RHD Saldana Emmanuel, Sales Stephanie, Salonga Cryscel, San Diego Phoebe, San Pedro Rina, Sanez Eric, Sanidad Erica, Santos Emmalene, Santos Jeniffer, Santos Joel, Santos Karen,Santos Mary Elaine
Elvie, 28 y/o housewife, dyspnea 3 days PTA Dental Procedure 2 days PTA • Cough productive of yellowish sputum accompanied by colds • Pricking chest pain radiating to the back lasting more than 30 minutes occurring even at rest • Fever at 38 degrees Celsius with joint pain and myalgia 1 day PTA Dyspnea Easy Fatigability Admission
Past Medical History • (+) frequent streptococcal throat infection in childhood • At age 16, diagnosed to have valvular heart disease with monthly injections of Benzathine Penicillin • Family History (+) hypertension – grandfather (+) heart disease - father
Physical Examination • Drowsy, in respiratory distress, prefers the semi-sitting position • BP: 130/60 mmHg PR: 124 beats/min • CR: 135 beats/min, irregularly irregular • RR: 40 cycles/min Temp: 38.5°C
Physical Examination • Cold, clammy extremities, no active dermatoses • No nasoaural discharge, with alar flaring • Moist buccal mucosa, hyperemic posterior pharyngeal wall, tonsils not enlarged • Supple neck, distended neck veins at 4-5cm at 30°angle • Symmetrical chest expansion, (+) supraclavicular retractions, coarse crackles over both lung fields
Physical Examination • Dynamic precordium, AB at 6th LICS AAL • (+) heave at the left lower parasternal area • (++) impulse at the 2nd LICS, • On auscultation at the apex, S1 was noted to vary in intensity, followed by a grade 3/6 holosystolic murmur that radiates to the axilla, S2 is normal followed by an opening snap and a grade 3/6 diastolic rumbling murmur • At the base, the pulmonic component of S2 is loud with a grade 3/6 diastolic blowing murmur
Physical Examination • Globular abdomen, liver is palpable • Extremity: grade 2 bipedal edema
Laboratory and Ancillary Tests • Chest X-ray: • Cardiomegaly with features of mitral valve pathology • Pulmonary edema • Haziness at right paracardiac border • ECG: • Atrial Fibrillation with rapid ventricular response • Non-specific ST-T wave changes • 2D-Echo: • Mitral Stenosis, moderate to severe • Mitral regurgitation, moderate • Aortic regurgitation, moderate • LV and RV dilatation • Dilated LA and RA with no evidence of thrombus • Dilated main pulmonary artery
Diagnosis • Rheumatic Heart Disease, active • Mitral stenosis, moderate to severe; Mitral regurgitation, moderate; Aortic regurgitation, moderate; LV and RV dilatation; Dilated LA and RA with no evidence of thrombus; Dilated Main Pulmonary Artery; Pulmonary Hypertension; Congestive heart failure in atrial fibrillation with rapid ventricular response • Class IV-D
Organism Factors • Acute Rheumatic Fever is caused by infection of the upper respiratory tract with any strain of group A streptococci. • A series of preceding streptococcal infections is needed to "prime" the immune system prior to the final infection that directly causes disease.
Host Factors • Findings of familial clustering of cases & concordance in monozygotic twins—particularly for chorea—confirm that susceptibility to ARF is an inherited characteristic. • HLA class II alleles • ↑levels of circulating MBL & polymorphisms of TGF-β1 gene and immunoglobulin genes
Immune Response • Epitopes present in the cell wall, cell membrane, and the A, B, and C repeat regions of the streptococcal M protein are immunologically similar to molecules in human myosin, tropomyosin, keratin, actin, laminin, vimentin, and N-acetylglucosamine. • Human molecules—particularly epitopes in cardiac myosin—result in T cell sensitization.
Immune Response • Laminin, another -helical coiled-coil protein like myosin and M protein, which is found in cardiac endothelium and is recognized by anti-myosin, anti-M protein T cells. • Antibodies to cardiac valve tissue cross-react with the N-acetylglucosamine of group A streptococcal carbohydrate, and there is some evidence that these antibodies may be responsible for valvular damage.
Mitral Stenosis • Inspection • malar flush with pinched and blue fascies • Palpation • Arterial pulse amplitude decreased • RV tap along left sternal border signifies enlarged RV, diastolic thrill at cardiac apex • Auscultation: • S1 accentuated and delayed and palpable at left sternal border • S2 closely split with accented P2 • OS readily audible in expiration • Follows P2 closely, followed by a low pitched, rumbling diastolic murmur heard best at apex and does not radiate • Soft grade 1 or 2/6 murmur heard at apex or left sternal border • Hepatomegaly, ankle edema, ascites and pleural effusion if with RV failure
Mitral Regurgitation • Usually asymptomatic for chronic mild-moderate MR • Palpation • Arterial pressure usually normal but may show a sharp upstroke • Systolic thrill at cardiac apex • Palpable rapid filling wave (S3) • Apex beat displaced laterally • In acute severe MR • Reduced arterial pressure • Normal or increased jugular venous pressure • Apical impulse not displaced • Auscultation • Grade 3/6 holosystolic high-pitched decrescendo, my obliterate S2 • Radiates from apex to base or to left axilla • Absent or soft S1 • Premature A2 resulting in wide but physiologic splitting of S2 • S3 often present • S3-S4 on those with severe MR
Aortic Regurgitation • Inspection • Jarring of the entire body and bobbing motion of the head with each systole • Abrupt distention (water hammer pulse) and collapse of large arteries during late sytole and diastole (Corrigan’s pulse) • Alternate flushing and paling of the skin at the root of the nail (Quincke’s pulse) • Booming sound on femoral artery ( Traube’s sign)
Aortic Regurgitation • Palpation • Elevation of systolic pressure (300 mmHg) • Depression of diastolic pressure • LV impulse is heaving and displaced laterally and inferiorly • Palpable diastolic thrill along the left sternal border, systolic thrill in suprasternal notch transmitted in the carotid arteries • Auscultation • Murmur is high pitched, blowing, decrescendo diastolic murmur heard best in 3rd ICS along the left sternal border • Low pitched rumbling murmur at the apex (Austin Flint) • Soft S1, M1 and A2 often intensified • S3 and systolic ejection sound are audible • Occasionally S4 can also be heard • Auscultatory features are intensified by strenous handgrip, which increases sytemic resistance
AUSCULTOGRAM MR, MS, AR, AS
Differential Diagnosis for the Cause of Fever • Myocarditis • Pericarditis • Systemic Lupus Erythematosus (SLE) • Pneumonia • Pulmonary Tuberculosis (PTB)
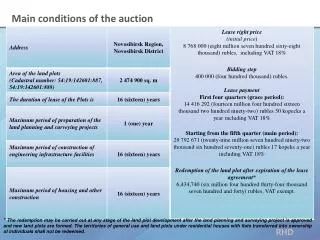
REVISED JONES CRITERIA2002-2003 WHO Criteria for the Diagnosis of RF and RHD Includes preceding streptococcal type A infection and a combination of major and minor clinical manifestations Harrison’s Principles of Internal Medicine, 17th ed.
REVISED JONES CRITERIA2002-2003 WHO Criteria for the Diagnosis of RF and RHD MAJOR MANIFESTATIONS: • Carditis • Polyarthritis • Chorea • ErythemaMarginatum • Subcutaneous Nodules MINOR MANIFESTATIONS: • Clinical: fever, polyarthralgia • Labs: elevated ESR, C-reactive protein (Acute Phase Reactants) • ECG: prolonged P-R interval • SUPPORTING EVIDENCE OF A PRECEDING STREPTOCOCCAL INFECTION W/IN THE LAST 45 DAYS: • Elevated or rising anti-streptolysin O or other streptococcal antibody, or • (+) Throat culture, or • Rapid antigen test for group A streptococcus Harrison’s Principles of Internal Medicine, 17th ed.
REVISED JONES CRITERIA2002-2003 WHO Criteria for the Diagnosis of RF and RHD DIAGNOSTIC CATEGORIES Primary Episode of Rheumatic Fever 2 Major OR 1 Major + 2 Minor manifestations Plus evidence of preceding group A streptococcal infection Recurrent attack of RF in a patient without established RHD 2 Major OR 1 Major + 2 Minor manifestations Plus evidence of preceding group A streptococcal infection Recurrent attack of RF in a patient with established RHD 2 Minor manifestations Plus evidence of preceding group A streptococcal infection Harrison’s Principles of Internal Medicine, 17th ed.
REVISED JONES CRITERIA2002-2003 WHO Criteria for the Diagnosis of RF and RHD DIAGNOSTIC CATEGORIES Rheumatic Chorea Insidous onset rheumatic carditis Other major manifestations or evidence of group A strep. infection not required • Infective endocarditis should be excluded. Chronic valve lesions of RHD Do not require any other criteria to be diagnosed as having rheumatic heart disease • Congenital heart disease should be excluded. Harrison’s Principles of Internal Medicine, 17th ed.
REVISED JONES CRITERIA2002-2003 WHO Criteria for the Diagnosis of RF and RHD “Probable Rheumatic Fever” • with polyarthritis (or with only polyarthralgia or monoarthritis) and with several (3 or more) other minor manifestations, plus evidence of recent group A streptococcal infection. • may later turn out to be rheumatic fever • advise regular secondary prophylaxis, follow up closely and do regular heart examination (esp. in vulnerable age groups in high incidence settings) Harrison’s Principles of Internal Medicine, 17th ed.
The Duke Criteria • The diagnosis of infective endocarditis is certain only when vegetations obtained are examined histologically and microbiologically. • Duke criteria is based on clinical, laboratory and echocardiographic findings. • 2 major criteria, 1 major + 2 minor criteria, or 5 minor criteria allows a definitive diagnosis.
The Duke Criteria • The diagnosis of infective endocarditis is rejected if: • Alternative diagnosis is established • Symptoms resolve and do not recur within 4 days or less of antibiotic therapy • Surgery or autopsy after 4 days or less of antimicrobial therapy yields no histologic evidence of endocarditis
The Duke Criteria • Illnesses not classified as definite endocarditis or rejected are considered possible cases when either 1 major + 1 minor citeria or 3 minor criteria are identified. • To fulfill a major criterion, the isolation of an organism that causes both endocarditis and bacteremia in the absence of endocarditis must take place repeatedly and in the absence of primary focus of infection.
The Duke Criteria • Organisms that rarely cause endocarditis but commonly contaminate blood cultures must be isolated repeatedly if their isolation is to serve as a major criterion.
The Duke Criteria • Major Criteria • Positive Blood Culture • Typical microorganisms from two separate blood cultures* • Persistently positive blood culture, defined as recovery of a microorganism consistent w/ infective endocarditis from: • Blood cultures drawn >12 hrs apart • All of three, majority of four or more separate blood cultures, with first and last drawn at least 1 hr apart • Single positive blood culture from Coxiellaburnetti or phase I IgGtiter > 1:800
The Duke Criteria • Evidence of Endocardial Involvement • Positive Echocardiogram • Oscillating intracardiac mass on valve or supporting structures or in the path of regurgitant jets or in implanted material, in the absence of an alternative anatomic explanation • Abscess • New partial dehiscence of prosthetic valve • New valvular regurgitation*
The Duke Criteria • Minor Criteria • Predisposition* • Fever >/= 38°C* • Vascular phenomena* • Immunologic phenomena* • Microbiologic Evidence*