Download
1 / 24
310 likes | 748 Views
HYPOTHYROIDISM. Dr Rona. H ypothyroidism. Common endocrine disorder of childhood Congenital/acquired. Hypothyroidism. Primary congenital &acquired Secondary

E N D
HYPOTHYROIDISM Dr Rona
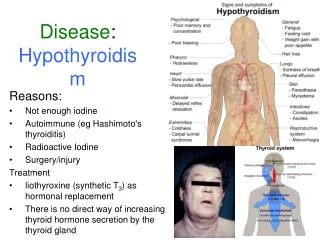
Hypothyroidism Common endocrine disorder of childhood Congenital/acquired
Hypothyroidism • Primary congenital &acquired • Secondary - due to deficiency of TSH/TRH - Hypopituitarism
Congenital hypothyroidism • Familial/sporadic • 85%cases-dysgenesis(manifests at birth) • 10-15%cases-inborn errors of thyroid hormone synthesis(often present later in infancy)
Congenital hypothyroidism • Etiology 1.dysgenesis:aplasia, hypoplasia, ectopic thyroid 2.inborn errors of thy: hormone synthesis 3.insensitivity/resistance to thy:hormone 4.maternal medication-radioiodine,PTU, Carbimazole
Clinical features(when to suspect?) • Prolonged physiological jaundice • Constipation • Lethargy • Feeding problems • Large tongue • Open posterior fontenel&wide open cranial sutures • Skin-dry,thick&coarse,cool&mottled
abdomen is large • sleep most of the time • Cry little, feed poorly &often get choking spells during feeding • Resp difficulties-noisy breathing, nasal obstruction&apnea • Hypothermia • Umbilical hernia
By the age of 8-10 wks characteristic coarse facial features become evident • Puffy face, swollen eyelids • Widely separated eyes, narrow palpebral fissures • Broad nose ,depressed nasal bridge • Open mouth, broad thick protuberant tongue
Neck is short and thick • Supraclavicular pad of fat may be present • Voice is hoarse • Skin-pale yellow, dry scaly&thick • Hair-sparse,coarse&brittle • Muscles are flaccid&markedly hypotonic
Marked physical and mental retardation • Social smile is delayed • Dentition &skeletal maturation is also significantly delayed • Pulse is slow, cardiomegaly &heart murmurs may be present • Refractory anemia is common
Acquired hypothyroidism • Etiology • Iodine deficiency • Hashimoto thyroiditis • Irradiation • Surgical ablation • Ingestion of goiterogens • Drug induced-iodides,PTU,Carbimazole.Li
Acquired hypothyroidism • Symptoms depend upon the severity and duration of thyroid dysfunction • Onset is insidious • Growth velocity is low;child appears short and stocky with disproportionately large head&trunk as compared to limbs
Expression is dull. • face appears puffy, skin and s/c tissue are thick and pigmented-myxedematous appearance • Child is lethargic with cold intolerence • Pulse rate & BP is low • Muscles flabby & hypotonic, rarely pseudo hypertrophy
Puberty is usually delayed. Galactorrhoea(increased prolactin secretion),sexual precocity may be seen • Goiter is frequently encountered
Investigations • Radiologicalretarded osseous devpmt. X-ray knee: absence of distal femoral epiphysis at birth, punctate epiphyseal dysgenesis • TFT T4, T3 low and TSH high in secondary hypo: TSH normal • Normal T3-60to80ng/dl,T4-5to12.5microgm/dl, TSH-2to4 IU
ECG- low voltage waves • Serum cholesterol-high • Imaging studies-USS and radio isotope scan : to identify anatomical and functional status of gland • Thyroid antibody studies-to identify auto immune thyroiditis
Neonatal screening • Measurement of TSH and T4 values using cord blood samples on filter paper • Infants with low T4 levels with elevated TSH are identified and recalled for repeat T4 and TSH measurements • Low T4 and elevated TSH- primary hypo: • Low T4 and TSH-Ix for TBG deficiency/sec hypothyroidism
Management • Sodium levothyroxin[100 microgm tab] is the treatment of choice • 0-3months of age10-15microgm/kg/day • 3-6months of age8-12microgm/kg/day • 7-12months of age6-8microgm/kg/day
1-5years4-6microgm/kg/day • 6-12years3-5microgm/kg/day • >12years2-4microgm/kg/day • Roughly 5-10microgm/kg/day decreases with advancing age
Better administered as a single dose early morning in empty stomach for maximum absorption • Start with smaller dose and gradually increase to optimal requirement • Neonates and children <1 year should receive therapy immediately
In children with secondary hypothyroidism cortisol replacement should be initiated before thyroid replacement thyroxine induces increased metabolism of steroid hormones
Therapy should be monitored by assessment of • Clinical symptoms • Gain in weight • Improvement in mental performance • Periodic thyroid function tests
TFT is done 4wks after initiation of treatment in newborn • If normal once a year monitoring with adjustment of dose for age/wt . • Skeletal maturation should be monitored