Download
1 / 35
360 likes | 534 Views
Case Discussion Pompe Disease 2003. 06. 30. Ri 許哲偉 Ri 李秉學. Brief History. This is a 1-year-old boy, G1P1, GA 39+5 wk, NSD, BBW 3178 gm. When he was 2 months old in Sep., 2002, he had cough, rhinorrhea, decreased appetite and activity, and he was admitted to 中國 hospital.

E N D
Case DiscussionPompe Disease2003. 06. 30. Ri 許哲偉 Ri 李秉學
Brief History • This is a 1-year-old boy, G1P1, GA 39+5 wk, NSD, BBW 3178 gm. • When he was 2 months old in Sep., 2002, he had cough, rhinorrhea, decreased appetite and activity, and he was admitted to 中國 hospital. • Cardiomegaly and hypotonia were noted and Pompe’s disease was suspected.
Brief History • 9/19/2002, in NTU, liver enzyme, cardiac enzyme, LDH level all increased. • Echo: hypertrophic cardiomyopathy、moderate LVOT obstruction, severe MR, mild TR, PFO. • Enzyme assays of lymphocyte, skin fibroblast and urine revealed prominent decreased α- glucosidase level.
Chief Complaint • High fever (40℃) with tachycardia for 2 days. • Acrocyanosis、chills、tachypnea、decreased urine output、dry lips were also noted. • Low grade fever with productive cough for 3 wks. Present Illness
Glycogen Storage Disease • Inherited disorders affecting glycogen metabolism. • Virtually all enzymes involved in its synthesis, degradation, and regulation cause some type of GSD. • Abnormal quantity and quality of glycogen. • Classified by organ involvement and clinical manifestation into liver and muscle glycogenoses.
Glycogen Storage Disease • More than 12 forms of glycogenoses. • 1/20,000 in live births. • Most common in childhood Deficiency of G-6-P (type I), lysosomal acid α- glucosidase (type II), debrancher (type III), and liver phosphorylase kinase. • Most common in adulthood Myophosphorylase deficiency (type V)
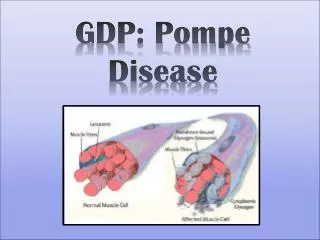
Pompe Disease (Type II) • Deficient activity of lysosomal acid α-1,4 glucosidase (acid maltase). • Accumulation of glycogen in lysosomes. • 1/50,000 in live births without ethnic prediction. • An autosomal recessive disorder, chromosome 17q23.
Clinical Manifestations Infantile form • Most severe, prominent cardiomegaly, hypotonia, and death prior to 2 yr of age. • “Floppy baby,” feeding difficulties, macroglossia, hepatomegaly, and heart failure due to hypertrophic cardiomyopathy. • ECG: high-voltage QRS, shortened P-R interval. • Death results from cardiorespiratory failure or aspiration pneumonia.
Clinical Manifestations Juvenile form • Delayed motor milestones, difficult walking, followed by swallowing difficulties, weakness of proximal muscle and respiratory muscle. • Death from respiratory failure before 20 yrs old. • Cardiomegaly is variable, and overt cardiac failure.
Clinical Manifestations Adult form • Slow progressive myopathy without cardiac involvement. • Onset between 2nd and 7th decades. • Proximal muscle weakness with trunk involvement. (pelvic girdle, paraspinal muscle, diaphragm are the most seriously affected) • Initial symptoms: respiratory insufficiency (somnolence, morning headache, orthopnea, and exertional dyspnea)
Laboratory Findings • Elevated levels of serum creatine kinase, AST, and LDH. • Muslce biopsy shows presence of vacuoles stained positive with glycogen. • Electron microscopy reveals glycogen accumulation within the membranous sac and in the cytoplasm. • EMG reveals myopathic features with excessive electrical irritability of muscle fibers.
Diagnosis • Decreased levels of acid α- glucosidase activity in muscle or cultured skin fibroblast. • Deficiency is more severe in the infantile form. • Prenatal diagnosis using amniocytes or chronic villi is available in the fatal infantile form.
Therapeutic approach to Pompe disease 1。Enzyme replacement therapy 2。Gene therapy
Gene therapy Provide a permanent internal source of enzyme
Gene therapy • Still in the early stage of investigation • Adenovirus carrying GAA(acid alpha glucosidase) was examined by intramuscular, intracardiac and intravenous administration • Correction of enzyme deficiency in In Vivo experiments
Major anesthetic problems • The cardiomyopathy • Oxygenation • Respiratory muscle weakness and the use of muscle relaxant
The cardiomyopathy • Massive infiltration of the ventricular wall may produce either a congestive or obstructive cardiomyopathy • Avoidance of myocardial depression and vasodilator • Using ketamine and sevoflurane seems to be reasonable
Oxygenation • Some children with Pompe disease have large toungues →might cause loss of airway control during anesthesia • Due to the cardiomegaly and weak respiratory muscle, patients have increased vulnerability to atelectasis and aspiration
Respiratory muscle weakness and muscle relaxants • Increased susceptibility to prolonged intubation after operation • Succinylcholine may cause rhabdomyolysis, hyperkalemia and cardiac arrest in children with undiagnosed myopathies.
Ureteroscopic removal of left ureteral lithiasis in a patient with acid maltase deficiency diseaseANESTH ANALG 1993;76:662-4 • A 71-year old patient with adult type of AMD come for removal of ureteral stone • Induction of anesthesia proceeded by propofol(100mg, IV) ,atracurim(35mg) • Ketorolac(60mg, IM) was injected • Anesthesia was maintained by 66% nitrous oxide and IV propofol infusion • Neuromuscular block was reversed by neostigmine and glycopyrrolate
Ureteroscopic removal of left ureteral lithiasis in a patient with acid maltase deficiency diseaseANESTH ANALG 1993;76:662-4 • The selection of drug was based on minimizing post.OP drowsiness, muscle weakness, and the respiratory depressant effect of anesthetics • Propofol was selected for its short recovery and post.operative stay • Narcotics were avoided and ketorolac was used for analgesia • Depolarizing muscle relaxant was considered unsafe
Prolonged respiratory depression after anesthesia for parathyroidectomy in patient with Juvenile AMD Journal of Clinical Anes.,Vol.8 1996 • 11 year-old boy with juvenile AMD and primary hyperparathyroidism undergoing parathyroidectomy • Anesthesia was induced by mask with enflurane, N2O and oxygen • Despite of avoidance of any muscle relaxant,the patient develop post.OP respiratory failure and was kept intubated until the 15th day after surgery
Conclusions • Avoid cardiac depressants and vasodilators • Keep PEEP and high FiO2 • Close monitoring post.OP condition